Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
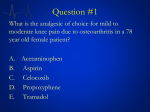
Pain Management in the Elderly Rog Kyle 10/7/11 Aging Q3 ACOVE #10 Background • Chronic pain (cancer and non-cancer) problematic in 25-50% of elders in the community • Osteoarthritis (and other musculoskeletal) is most common cause • Low back pain (LBP) most prevalent condition – 10 million Americans disabled • Others – Postherpetic neuralgia (PHN) – Painful diabetic neuropathy – Post stroke pain • Cancer pain – 80% of elderly with cancer report pain – Probably under detected and under treated – Deficiencies • Under documented • Under treated – opioids and non-opioids • Reporting by patients – Most feared complication of illness – Pain is the second leading complaint in physicians’ offices – Effects on mood, functional status, and quality of life – Associated with increased health resources use • Barriers to reporting – Cognitively impaired – More tests – Fear of medications – Fear of the cause for the pain – Complaining may effect quality of care – Believe nothing can or will be done • Hospitalized patients – No randomized trials – Prospective studies on cancer patients • Underestimate pain • Probably do not assess frequently enough Challenges in the elderly • • • • Comparatively little data Cognitive impairment and compliance Underreported by patients Drug-drug interaction and polypharmacy a serious concern • Reduced hepatic function, reduced renal function Mechanisms for pain • Nociceptive – Nociceptors = pain fiber sensitive to noxious stimuli • Somatic – injury to tissues, well localized • Visceral – injury to organs (stretch receptors), poorly localized • Neuropathic – Abnormal neural activity secondary to disease, injury, or dysfunction (allodynia). – Persists without ongoing injury (trigeminal neuralgia, DM neuropathy) – Types: • Sympathetic – from peripheral nerve injury with autonomic changes – “New” term – Complex Regional Pain Syndrome (CRPS) • Type I = RSD • Type II = causalgia • Peripheral autonomic pain – – Same but without autonomic change (PHN) • Central Pain (spinal cord injury) Pain pathways • Nociceptive fibers – afferent fibers to dorsal horn – Two types • A-delta – sharp pain (fast) • C polymodal – dull pain (slow) • Pathways • Nociceptive fibers – afferent fibers to dorsal horn – Two types • A-delta – sharp pain (fast) • C polymodal – dull pain (slow) • Pathways • Central processing – Interneurons between spinal cord/thalamus/cortex modulate pain and may be either excitatory of inhibitory – endogenous systems also control pain perception – opioid, noradrenergic (fight or flight), and serotonergic Mechanisms for chronic pain • • • • • • • • Peripheral sensitization Central sensitization Disinhibition Desensitization Ectopic excitability Structural reorganization Phenotypic switch of neurons Primary sensory degeneration Sensitization • Main cause for hypersensitivity to pain after an injury (nociceptive sensitizer) • Each has it’s own proposed mechanism at the cellular level – Peripheral – injury/inflammation releases cytokines, chemokines, bradykinin, histamine, prostaglandins – Central – amplifies info from nociceptors – NMDA receptor upregulated (controls pain – ketamine), GABA inhibition - disinhibition - “inhibits inhibition” Treatment – non drug strategies • Exercise – PT, OT, stretching, strengthening – general conditioning • Physical methods – ice, heat, massage • Cognitive-behavioral therapy • • • • Chiropracty Acupuncture TENS Alternative therapies – relaxation, imagery – herbals WHO Ladder (adapted for elderly) – Level 3 (severe pain): Strong • opioids—morphine, hydromorphone, • fentanyl, oxycodone ±adjuvants – Level 2 (moderate to severe pain): • Acetaminophen plus opioid (hydrocodone, • oxycodone, codeine); tramadol ±adjuvants, • Propoxyphene (X) – Level 1 (mild to moderate pain): • Acetaminophen, aspirin (X), nonspecific NSAIDs (X), • COX-2–specific NSAIDs±adjuvants Figure 1. WHO ladder (adapted for the elderly). Note: Therapies marked with an “X” are not appropriate for use in the elderly. Non-opioid options • • • • • • • • • • Acetaminophen Alpha-adrenergic agents Anticonvulsants Antidepressants Muscle relaxants Neuroleptic agents NMDA-receptor antagonists NSAIDs Oral local anesthetics Topical analgesics Acetaminophen • First line • 4000mg max – 2000mg recommended with etoh use, liver disease, elderly • Watch for other OTC’s containing acetaminophen Alpha-adrenergics • Epidural clonidine for neuropathic pain (FDA) • Tizanidine outside US Anticonvulsants • Neuropathic pain • Second gen may have fewer side effects (gabapentin, topiramate) • Many approved for HA/pain – – – – – – Carbamazepine (trigeminal neuralgia) Divalproex (migraine) Gabapentin (PHN) Pregabalin (PHN, diabetic neuropathy) Topiramate (migraine) Duloxetine (diabetic neuropathy, fibromyalgia, DJD) • Off label – Lamotrigine for HIV neuropathy (and others) – PDN • Carbamazepine, phenytoin, gabapentin – Chronic musculoskeletal pain Antidepressants • Analgesia independent of antidepressant effects • Tricyclics (amitriptyline) for neuropathic pain – Nortriptyline has safer side effect profile in > 60 – Amitriptyline relatively contraindicated in elderly (cardiac, anticholinergic) • SNRI’s – Duloxetine, venlafaxine • Others – Bupropion, venlafaxine, duloxetine (neuropathic) • SSRI’s/SNRI’s not shown to have efficacy comparable to tricyclics TRICYCLIC SSRI Amitriptyline Desipramine Doxepin Imipramine Nortriptyline Fluoxetine Paroxetine Sertraline Fluvoxamine Citalopram *FDA approved for pain OTHER Venlafaxine Duloxetine* Trazodone Bupropion Muscle relaxants • Cyclobenzaprine – – – – Similar to tricyclic's Acute LBP (2 trials) Anticholinergic side effects, cardiac arrhythmia Avoid in elderly • Carisoprodol (meprobamate precursor) – Acute LBP – Dependency (physical, psychological), drowsiness • Metaxalone (Skelaxine) – Non-sedating, watch for liver tox • Baclofen – GABA agonist Neuroleptics • Fluphenaxine (Prolixin) – Not recommended NMDA receptor antagonists • Scientific promise – Dextromethorphan – Ketamine – Methadone – Memantine – Amitriptyline NSAIDS • 60 million Rx’s/yr (3.6 fold higher in elders) • Clinical efficacy of equipotent doses is similar • Individual responses highly variable – especially toxicity – cox-1 vs. cox-2 – naprosyn may have greatest relative cardiovascular safety profile – diclofenac - available as a topical patch for pain due to trauma and as a gel for treatment of painful joints – sulindac – increased hepatoxicity – indomethacin - GI and central nervous system adverse effects may be more frequent or severe than with other NSAIDs – ketorolac - Risk of gastropathy is increased when use exceeds five days – piroxicam – high GI toxicity – celecoxib – no antiplatelet function. Increased CV risk above 200mg/day • Generally indicated in mild to moderate pain • Mostly for pain of somatic origin although has a CNS effect as well • Each trial should last a couple weeks • May have an opioid sparing effect as adjunct • Protein bound – may interfere with other protein bound drugs (dilantin. coumadin) • Noted variability in the response to NSAIDS between patients – Does not appear related to serum concentrations – Degree of Cox inhibition doesn’t correlate with effect – Non-prostaglandin effects may predominate in some patients – Switching between classes of NSAIDS may be beneficial Topicals • Lidoderm – FDA approved for PHN (intact skin) – Often used in musculoskeletal pain • Diclofenac patch – Topical treatment of acute (short-term) pain due to minor strains, sprains, and contusions (bruises) • Capsaicin – Neurotransmitter depletion – PHN, musculoskeletal Tramadol • Mu receptor and SNRI effects • Effective in neuropathic pain, fibromyalgia, OA • Similar side effects to opioids – Seizures, suicide Benzodiazepines • Adjuvant only • Anxiolytic • Limitations – Sedation – Addictive potential – Respiratory depression – Avoid in elderly • Clonazepam – Effective in PHN and myoclonus Opioids • Role in treatment of pain is well established for acute pain, malignant pain and care of the terminally ill • Role in chronic non-cancer pain is more controversial • No specific studies have been performed in the elderly • Decision to begin long term opioid therapy in chronic, non-cancer pain “must be weighed carefully” • Most of the literature on opioid therapy consists of reports of surveys and uncontrolled case series • Most find that chronic pain can be controlled with nonescalating doses of opiates – up to 6 years of rx, 180 mg morphine – – – – Function is improved by pt report Cognitive function is preserved Ability to drive or operate machinery is preserved High drop out due to side effects (25%) • Establish diagnosis • Confirm inadequacy of nonopioid and nonmedical treatments • Ensure that the balance of risk and benefit favors treatment • Explain benefits and risks and clinic’s monitoring policies • Establish treatment goals • Request written consent or contract, when necessary Side effects • • • • • • • • • • Constipation Nausea, vomiting Sedation Impaired judgment Impaired psychomotor function Respiratory depression Hypotension Myoclonus GU Pruritus • Constipation – Fluids, fiber, stool softener, cathartic – methylnaltrexone • Sedation – Methylphenidate, modafinil • Dosing – no universal agreement – Start with lowest dose of short acting preparation – Up titrate no more often than weekly – Convert to sustained release formulations when possible (25-50% of 24 hour total) – Monitor for efficacy, side effects “Blue Sheet” Practice Partner Template – Is patient currently taking an opioid medication? <yes> <no> – If yes is clicked, then: • Is patient taking any adjuvant pain medications? <yes> <no> • Does patient report side effects? <yes> <no> • Based on pain assessment, plan to: (pick list of :) – Increase dosage of opioid pain medication – Decrease dosage of opioid pain medication – Add adjuvant pain medication – No changes planned to pain medication regimen Pain Management ACOVE starts on: October 24, 2011