Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
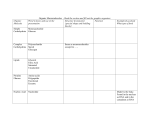
Nutritional Management of Diabetes at School Betsy Smith, MS, RD Children’s Hospital January 11, 2007 Nutrition Objectives • To provide nutrition guidelines for the school nurse working with children with diabetes • To describe the most popular methods of diabetes medical nutrition therapy • To describe and educate on the use of carbohydrate counting Outline • Professional guidelines • 2 Main types of MNT with pediatrics • Carbohydrate Counting • Making adjustments for exercise • Questions Goals of Medical Nutrition Therapy • To provide adequate energy to ensure normal growth & development • To facilitate changes in eating & physical activity habits to reduce insulin resistance • Attain & maintain optimal metabolic outcomes • Prevent & treat the chronic complications of diabetes Goals of Medical Nutrition Therapy • Improve health through healthy food choices & physical activity • Address individual nutritional needs • To provide self-management education for treatment of acute complications • To decrease diabetes risk by encouraging physical activity & promoting healthy food choices Medical Nutrition Therapy • Goal to achieve blood glucose goals without excessive hypoglycemia • Based on requirements for all healthy children & adolescents • Ensure adequate intake of essential vitamins & minerals Diabetes Classification Type 1 Diabetes • • • • • Idiopathic Autoimmune Beta cell destruction Autoantibodies Insulin dependent Clinical Presentation Type 1 Diabetes • • • • • • • Hyperglycemia Ketoacidosis Dehydration The “Polys” Nausea & vomiting Ill appearing Weight loss Diabetes Classification • • • • • Type 2 Diabetes Insulin resistance Deficient insulin secretion Obesity or increased body fat Elevated insulin levels Initially treated with diet, exercise, medications Clinical Presentation • • • • • • • Type 2 Diabetes Increased weight gain Ketonuria The “Polys” Hyperglycemia Elevated serum insulin Acanthosis nigricans Infections Medical Treatment of Diabetes • Target blood sugar range • Use of insulin Subcutaneous (SQ) injections Continuous SQ insulin infusion • Use of oral hypoglycemic agents • Weight management • Exercise • Medical nutrition therapy Weight Management for Type 2 Diabetes • Exercise can decrease insulin resistance & help with weight management • Weight loss can also improve lipid levels • Decrease risk for more immediate health risks • Slow rate of weight gain Weight Management for Type 2 Diabetes • 3 meals + 2-3 snacks a day should be encouraged • Consumption of more fruits & vegetables, whole grain products, lowfat dairy products • Facilitate behavior change • Identify barriers to success & help eliminate them ADA Exchange List • Developed in 1950, revised by ADA in 1995 • Lists of groups of measured foods that equal an “exchange” • Can be used for Type 1 & Type 2 • Alerts patient to fiber & sodium • Divides foods into 3 food groups • Carbohydrate • Meat & Meat Substitutes • Fat ADA Exchange List Advantages • Provides a framework for grouping foods • Emphasizes important nutritional management concepts • Can use nutrient values from food labels Not appropriate for use if the family cannot understand “exchanging” Carbohydrate Counting • Been around since 1920’s • Specifically focused on techniques to optimize blood glucose control • Used to match pre-meal insulin doses to the demand created by food • Other nutrition aspects must be addressed separately Carbohydrate Counting •Easier to learn than exchanges •Offers more variety in food choices •Provides a more accurate prediction of rises in blood sugar following a meal or snack •Allows utilization of food labels to make meal planning easier Carbohydrate Counting Three Levels •Basic - learn carbohydrate exchanges & consistent intake •Intermediate - learn to identify patterns in blood glucose levels that are related to food eaten, diabetes medications used, &/or physical activity and how to make adjustments Carbohydrate Counting • Advanced - learn how to adjust short-acting insulin to the carbohydrate content of meals (carbohydrate to insulin ratios) SO HOW DO YOU COUNT CARBOHYDRATES? IDENTIFY CARBOHYDRATE FOOD SOURCES MILK FRUITS STARCHES & STARCHY VEGETABLES The Fruit Group • Fresh fruit • Canned fruit (packed in lite syrup, juice or water) • 100% fruit juice (Labeled on container) • Dried fruit (raisins) The Starch Group • Starches (bread, pasta, rice, crackers, cereals, snack foods) • Starchy vegetables (corn, potatoes, dried beans, peas) The Milk Group • Milk • • • • (whole, 2%, 1%, skim, buttermilk) Yogurt Pudding Ice cream NOT CHEESE ! WHAT TO CONSIDER WITH CARBOHYDRATE • Used terms: sugars, starch, fiber • Factors that influence glycemic responses to foods: Amount of Carbohydrate Type of sugar Nature of the starch Cooking & food processing Food form BE FAMILIAR WITH HOW MUCH FOOD COUNTS AS A SERVING 1 CARBOHYDRATE SERVING = 15 GRAMS CARBOHYDRATE The Fruit Group • Fresh fruit 1 cup, 1/2 banana, 15 grapes, 1/8 cantaloupe, tennis-ball size piece • Canned fruit 1/2 cup • 100% fruit juice 4 ounces • Dried fruit 2 Tablespoons The Starch Group • Starches 1 slice bread, 1/3 cup rice, 1/2 cup pasta, 1/2 cup cereal, 1 small roll, 1/2 bun • Starchy vegetables 1/2 cup corn, potatoes, dried beans, peas The Milk Group • Milk 8 ounces • Yogurt 1 cup • Pudding & ice cream 1/3 - 1/2 cup READ THE NUTRITION FACTS LABELS! 3 THINGS TO READ ON A LABEL • Serving Size • Total Carbohydrate • Total Fat How Meal Plan Developed for Each Child • Based on age & ideal body weight in kilograms • Pattern of growth & weight gain • Typical food intake at home • Food history & activity patterns • Time & place of all meals & snacks • Home & school schedule during week Carbohydrate Counting: Suggested Education Progression • Initial session Diet goals and rationale Healthy nutrition Balanced meals Timing/consistency of meals Carbohydrate, protein, fat sources & effects on blood sugar levels Concentrated sweets/free foods Basic level of carbohydrate counting Carbohydrate Counting: Suggested Education Progression • Follow-up (initial 1 to 2 months, at 6 months, yearly full nutrition assessment) Individualized meal plan based on clinical goals and patient/family readiness & motivation Meal Plans at School • Prescribed carbohydrate grams for meals and snacks • Not every child with diabetes will have a meal plan • Usually prescribed at diagnosis or clinic visit, cannot be prescribed over the phone • Sent to nutritionist of Child Nutrition Program, who sends it to the school Exercise Guidelines for Type 1 Diabetes • Blood glucose monitoring • Precautions to avoid hypoglycemia • Food intake may need to be increased • Fluid intake is essential Exercise Guidelines for Type 1 Diabetes • Carry adequate ID & a source of fastacting carbohydrate • May require a decrease in insulin • Continue monitoring blood glucose after exercise is completed General Guidelines For Making Food Adjustments Types of Exercise If Blood Sugar Is: Less than 80 Increase Food Intake By: 10-15 g CHO/hour Above 80 Not needed Jogging, swimming, golf Less than 80 25-50 g CHO/hour 80-170 10-15 g CHO/hour Football, soccer, basketball, cheerleading Less than 80 45 g CHO/hour 80-170 20-45 g CHO/hour Walking, leisure bike Parties at School • Can still participate and eat food at parties! • Communicate with parent ahead of time – Can plan to change insulin dose to cover party food – Plan to have party around time of snack • Encourage teacher or parents to provide healthy snacks at parties, sugar-free hard candy and lollipops • Use fat-free whipped topping as icing on cakes or cookies Questions