Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
PPREPARED BY
ALPHONSA SEBASTIAN
OR DEPARTMENT
DEMOGRAPHIC DATA
NAME
: MR.M. K. Z
AGE/SEX
: 24YRS/MALE
DATE OF ADMISSION
: 24/02/2013
DIAGNOSIS
: HAEMOPERITONIUM
SURGERY
ON
: 24/02/2013
SURGICAL INTERVENTION : EXPLORATORY
LAPROTOMY WITH SPLEENECTOMY
DISCHARGED ON
: 02/03/2013
• Patient is conscious.
• Looks weak and fatigue
• His vital signs are
•120/67mmof hg
•P/R
:82/mt
•RR
: 22/mt
•SPO2 :98%
•
Skin is warm .
• Light complexion.
• Warm to touch.
•
Absence Of Dandruff.
• Able to move both eyes
• No redness.
• Hair Is Equally Disrtibuted.
• Pupils reactive to light.
• Patients pinna is same colour as
• Skin,aligned with eye level .
• Able to hear sounds clearly .
• No discharges.
• No ulcers present in the mouth.
• Oral cavity is pale in colour.
• Lips pale and dry.
fascial.
.
• Teeth is propely aligned with no dentures.
• No tenderness of node.
• The Thorax Is Symmetric On Inspection
• Tenderness Of Abdomen present on palpation.
.
• No deformities of upper and lower limbs.
• Absence Of Chest Pain .
• Heart sounds are clear.
• Upon auscultation his Bp is 132/78mmofhg
• With foley catheter fr.16
.
Patient Is Mentally Alert And Oriented With
Circumstances.
•
Able To Follow Commands.
•
No neurovascular deficit.
No past surgical history.
•
Ct abdomen with contrast
• Ct abdomen with out contrast
• Blood investigations
INVESTIGATIONS
RESULTS
NORMAL VALUE
WBC
20.63
4.23-9.07
NEUT
76.6
34-67.9
RBC
2.68
4.63-6.08
HB
8.2
13.7-17.5G/DL
PLT
236
163-337
PT
APTT
16.3
30
10.9-16.3secs
27-39secs
Urea
Creatinine
Sodium
Pottassium
23.2
121
140
5.1
3.2-7.1mmol/L
46-110mmol/L
137-145mmol/L
3.5-5.1mmol/L
Chloride
114
98-107mmol/L
CBC
ABO RH
O +ve
SURGICAL INTERVENTION
EXPLORATORY LAPAROTOMY
WITH SPLENECTOMY
NAME OF THE
MEDICINE
DOSE
ROUTE&
ACTION
INJ.PREMOSAN
10mg
IV /BID
Antiemetic
INJ.RISEK
40mg
IV/OD
H2receptor
antagonist
INJ.CIPROXIN
200mg
IV/BID
Antibiotic
INJ.FLAGYL
500mg
IV/BID
Antibiotic
INJ.TRAMADOL
50mg
IM/TID
Analgesic
FREEQENCY
Splenectomy is a surgical procedure to
Remove spleen — an organ that sits under
rib cage on the left side of abdomen.
TYPES OF SPLENECTOMY
1. Minimally invasive (laparoscopic) splenectomy
During laparoscopic splenectomy, the surgeon makes
four small incisions in abdomen. A tube with a tiny video
camera is inserted into abdomen through one of the
incisions. Surgeon watches the video images on a
monitor in the operating room as special surgical tools
are inserted through the other incisions in abdomen and
spleen is removed. The incisions are then closed.
2 . Traditional (open) splenectomy.
During open splenectomy surgeon makes an
incision in the middle of abdomen. Muscle and
other tissue are moved aside to reveal spleen.
surgeon then removes the spleen, and closes the
incision.
Laparoscopic splenectomy isn't appropriate for
everyone. A ruptured spleen usually requires open
splenectomy. In some cases surgeon may begin with
a laparoscopic approach and find it necessary to
make a larger incision because of scar tissue from
previous operations or other complications.
•Receive blood transfusions before surgery to ensure have
enough blood cells following removal of spleen.
•Receive a pneumococcal vaccine to help prevent
infection after spleen is removed.
•Temporarily stop taking certain medications and
supplements.
•Avoid eating or drinking for a certain amount of time
before the surgery.
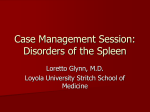
The spleen is an organ shaped like a shoe
that lies relative to the 9th and 11th ribs
and is located in the left
hypochondrium and partly in the
epigastrium. Thus, the spleen is situated
between the fundus of the stomach and the
diaphragm. The spleen is very vascular and
reddish purple in color; its size and weight
vary. A healthy spleen is not palpable.
The spleen is a lymphatic organ interposed in the blood
stream. The surface projection of the longitudinal axis of
the spleen is the tenth rib. It is concealed anteriorly by the
greater curvature of the stomach and the left colic
(splenic) flexure. Its weight varies from 50 to 250g.
HILUM
The hilum can be found on the inferomedial part of the gastric impression (see
the image above). The hilum transmits the splenic vessels and nerves and
provides attachment to the gastrosplenic and splenorenal (lienorenal)
ligaments
PERITONEAL RELATIONS
The spleen is surrounded by peritoneum and is suspended by multiple ligaments,
as follows:
• The gastrosplenic ligament
•
The splenorenal ligament
• The phrenicocolic ligament
VISCERAL RELATIONS
The visceral surface of the spleen
contacts the following organs:
•
Anterior surface of the left kidney .
•
Splenic flexure of the colon
•
The fundus of the stomach
•
Tail of pancreas
FUNCTIONS OF SPLEEN
There are three major functions of the spleen and these
are handled by three different tissues within the spleen.
Concerned with phagocytosis of erythrocytes and cell debris from
the blood stream. This same tissue may produce foci of haemopoiesis
when rbc's are needed.
Along with the power of the spleen to contract, provides a method for
expelling the contained blood to meet increased circulatory demands in
certain animals.
Provides lymphocytes and a source of plasma cells and hence
antibodies for the cellular and humoral specific immune defenses
Vascular supply
The splenic artery supplies blood to the spleen.This artery is the largest branch
of the celiac trunk and reaches the spleen's hilum by passing through the
splenorenal ligament. It divides into multiple branches at the hilum.It divides
into straight vessels called penicillin ellipsoids, and arterial capillaries in the
spleen.
NERVE SUPPLY
Sympathetic fibers are derived from the celiac plexus.
LYMPHATIC DRAINAGE
Proper splenic tissue has no lymphatics; however,some arise
from the capsule and trabeculae and drain to the
pancreaticosplenic lymph nodes.
VENOUS DRAINAGE
The splenic vein provides the principal venous drainage of the
spleen. It runs behind the pancreas (after forming at the hilum)
before joining the superior mesenteric vein behind the neck of
the pancreas to form the portal vein. The short gastric, left
gastro-omental, pancreatic, and inferior mesenteric veins are its
tributaries
VENOUS
DRAINAGE
•Ruptured spleen.
If spleen ruptures due to a severe abdominal injury or because
of enlargement of spleen (splenomegaly), the result may be life-threatening,
internal bleeding.
•Blood disorder.
Idiopathic thrombocytopenic purpura (ITP),
Polycythemia vera,
Thalassemia and sickle cell anemia.
• Cancer.
Chronic lymphocytic leukemia,
hodgkin lymphoma and non-hodgkin lymphoma
Hairy cell leukemia.
• Infection.
A severe infection or a large collection of pus surrounded by
inflammation (abscess) within your spleen that doesn't respond to
other treatment may require splenectomy
• Cyst or tumor.
Noncancerous cysts or tumors inside the spleen may
require splenectomy if they become large or are difficult to
remove completely.
•
Blood vessel problems
Aneurysm in the spleen's artery
Blood clot in the spleen's blood vessels
Infections
• Streptococcus pneumonia
• Neisseria meningitides
• Haemophilus influenzae
These bacteria cause severe pneumonia,
meningitis, and other serious infections.
Vaccinations to cover these bacteria should be
given in patients without a spleen.
Other
complications
splenectomy include:
•
•
•
•
•
•
related
to
Blood clot in the vein that carries blood to the
liver
Hernia at the incision site
Infection at the incision site
Inflammation of the pancreas (pancreatitis)
Lung collapse
Injury to the pancreas, stomach, and colon
Call the doctor right away if you have any of the
following after a splenectomy
• Bleeding.
:
•
•
•
•
•
•
•
Chills.
Cough or shortness of breath.
Difficulty eating or drinking.
Increased swelling of the abdomen.
Pain that doesn't go away with
prescribed medications.
Increasing redness, pain, or discharge (pus) at the incision site.
Nausea or vomiting that persists.
• Fever over 101 degree.
Hospitalization for 2 days .
• Iv fluids .
• Antibiotics .
• To guard against infections, doctor may recommend a
pneumonia vaccine, as well as yearly flu vaccines.
• Immunizations against pneumococcus species as a
routine of postoperative management. Immunization
should be administered anywhere from 24 hours after
injury to 2 weeks.
•
Tachypnea, ronchi, crackles, cloudy foul smelling urine, urgency
frequency, irritation ulcers of oral, vaginal or other mucosa;
redness or drainage from wound or invasive sites.
•
Hypotension, shock-like state. Indicates potential for
meningeal infection .
Monitor, Describe, Record
• White blood cells increases, urine, blood and wound cultures
and sensitivities. WBC of > 10,000 cu/mm positive cultures for
infectious organisms.
• Immunoglobulins. IgM decreases, IgG ad IgA within normal
ranges indicating deficiencies.
• Vital signs and temperature every four hours. Indicates
presence of infection
•
Antibiotics specific to identified infectious agent.
•
Antipyretic (acetaminophen.
• Handwash techniques before giving care.
• Aseptic technique for any invasive procedures.
•
Adequate fluids, nutritional and activity support.
• Meticulous mouth and perineal care.
High risk for infection related to inadequate secondary
defenses by immunosuppresion resulting from decreased
immunoglobulins
Acute pain related to surgical incision
Risk for defficient fluid volume related to heamorrhage caused by
surgery of highly vascular organ.
Knowledge deficit regarding treatment regimen and post op care .
ASSESSMENT NSG DIAGNOSIS
SUBJECTIVE
High risk for
infection
I have fever
related to
and chilling
as verbalized inadequate
by the patient secondary
defenses by
OBJECTIVE
immunosuppr
esion
• Elevated
resulting from
temperature decreased
P/R-126/mt
immunoglobul
TEMP-38.6C
ins.
RR-24/mt
Chills
Tachypnea
• Cloudy foul
smelling
urine
• Redness
or drainage
from wound
or invasive
sites.
PLANNING
After series
of nursing
interventions
the client
should
manifest no
signs of
infection .
INTERVENTION
RATIONALE
1.Asses for
1.High grade fever
Temperature elevation indicates infection
above 101 fh,chills
2. Assess for
tachypnea, crackles,
cloudy foul smelling
urine, urgency
frequency.
3.Asses for
hypotension, shocklike state.
2. Indicates
pneumococcal
infection or
overwhelming
infection.
EVALUATION
After 12 hrs of
nursing
interventions the
goals were fully met
as evidenced by…..
Absence of
infection evidenced
by
1 .Temperature,
3.Indicates potential
for meningeal
infection.
white blood cell,
urinalysis, cultures
within normal
4.Monitor urine, blood
4.To identify the
ranges
and wound cultures
presence of infectious
[Temp-36.6c
and sensitivities.
organisms.
Pr/82bpm,rr-20/mt
}
5.Administer specific
antibiotics
{INJ:CIPROXIN 200MG IV
,BID.
INJ:FLAGIL 500MG IV,BID}
6.Administered
antipyretics
{INJ:PERFALGAN 1GM
STAT}
5.Acts to destroy
microorganisms by
inhibiting cell wall
synthesis.
6.Reduces fever by
inhibiting heatregulating center.
2.Breath sounds,
urinary pattern,
mucous membranes
within baseline
levels.
Instruct The Patient
• Take short walks on a level surface
• Don’t overexert to the point of fatigue.
• Limit stair climbing to no more than once or twice a day. Climb steps slowly
and stop to rest every few steps
• Don’t lift anything heavier than 10 pounds or push a vacuum cleaner for 4 to 6
•
weeks after surgery.
Don’t drive until after first doctor’s appointment after surgery
.
• Get medical attention even for mild illnesses such as sinus problems or
• colds.
.
• Take antibiotic medication after surgery as directed by doctor
• Be sure to tell all your healthcare providers that he doesn’t
have a spleen
• Wash incision site with soap and water and pat dry.
• Check incision every day for redness, drainage, swelling, or
separation of the skin.
• Take the medications exactly as directed. Don’t skip doses.
• Don’t take any over-the-counter medication unless the doctor tells
to do so.
• Check temperature each day for 1 week after surgery.
• Make a follow-up appointment as directed.
•
A case of RTA patient who underwent splenectomy as an emergency procedure
on 24/02/13.
•
Splenectomy is a surgical procedure to remove spleen an organ that sits under
rib cage on the left side of abdomen.
•
The two types of splenectomy are open splenectomy and laproscopic
splenectomy . A ruptured spleen usually requires open splenectomy.
•
Patient was discharged on 02/03/13 .
•
He was instructed about the follow up care and has been explained he is prone
to infection as he does not have a spleen.
Bibliography
• Lippincott manual of nursing
practice 9 th edition
• www.mayoclinic .com
• Wikipedia
• Grays anatomy and physiology