Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
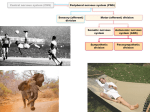
ANS & Heart The structures and functions of the sympathetic and parasympathetic systems on the heart differ in various ways. Presympathetic fibres originate in the brainstem, synapsing with preganglionic fibres in T1-5 spinal cord segments bilaterally. Each preganglionic fibre synapses with a postganglionic fibre located in the stellate ganglion of the sympathetic chain. These fibres innervate the ventricles, the SAN and the AVN in the heart. In the parasympathetic system, preganglionic fibres of the vagus nerve synapse with postganglionic fibres located in the heart tissue. The postganglionic fibres only innervate the SAN and AVN. Sympathetic outflow to the heart causes positive chronotropy, ionotropy, lusotropy and dromotropy (increased AVN conduction). As a result there is slow onset tachycardia, an increased gradient and size of AP and an increased if current. The parasympathetic system induces the opposite effects; however, the two systems do not act symmetrically on the heart. While parasympathetic outflow reduces the if current by causing MDP to be more negative (thus requiring the current more time to reach threshold) the sympathetic system does not affect MDP. Parasympathetic stimulation also induces hyperpolarisation and bradycardia. Heart rate is determined by the duration of pacemaker potential decay i.e the time taken for the potential to become less negative due to Na and Ca influx and inhibition of IK. The duration of this also determines the duration of diastole. Sympathetic outflow decreases the pacemaker potential decay via the following mechanism: NE and E activate beta receptors coupled to Gs which activates AC and increases cAMP elvels in the ell. CAMP activates PKC which phosphorylates effector proteins, resulting in an increased if current rate and in L-type Ca channel activity. As a result, the rate of depolarization at phase O increases and there is a positive chronotropic effect. The parasympathetic system increases the pacemaker potential decay via two mechanisms. ACh directly activates Ikach channels (normally background IK inactive) resulting in an influx of K ions, hyperpolarizing the cell. ACh also binds M2 receptors that are coupled to Gi and inhibit AC. Resulting cAMP levels are lowered which decrease L-type Ca channel activity, the if current and result in negative chronotropy. Sympathetic outflow (in the form of isoprenaline, NE or E) causes a positive ionotropic effect on ventricular CMCs. This is done by increasing intracellular Ca levels. Increasing SERCA activity also causes positive lusotropy as more Ca is taken up into the SR. SERCA is also controlled by the RyR channel on SR membrane that is phosphorylated by PKA, increasing its Ca pump activity. Presynaptic inhibition of both autonomic nervous systems ensures their reciprocal activity. Figure 3 shows reciprocal inhibition. At rest HR is lowered from 100 bpm to 70bpm by vagal tone. During exercise sympathetic activity increases and parasympathetic activity decreases. ANS structure The peripheral nervous system is the conduit between CNS and the external/internal environment. ANS consists of preganglionic neurons that originate in the CNS and synapse onto postganglionic nerves on ganglions, which then innervate effector organs. These connections can be inhibitory or excitatory via nerve endings and varicosities but there are no motor end plates or NMJs like in the somatic NS. ANS action is spontaneous and involuntary and the two systems antagonise each other but remain in balance. Figure 1 – structure of NS. Exception to the model: skeletal muscle of the diaphragm/intercostals innervated by autonomic control. Sympathetic preganglionic fibres originate in T1-12 and L1-3 regions of the SC (in lateral horn), are short, myelinated and synapse with and release ACh onto long (unmyelinated) postganglionic fibres at the paravertebral ganglia which then release NE onto effector organs. Long parasympathetic preganglionic fibres form the vagus and pelvic nerves that originate in the brainstem, synapse with postganglionic fibres on fewer effector organs, releasing ACh onto them. The postganglionic fibres also release ACh and mediate parasympathetic effects. Major effects of the sympathetic system are: increased adrenaline release from adrenal medulla; increased renin release; ejaculation in males; arteriolal vasoconstriction via alpha1/2 activation; minor dilation of skin and skeletal muscle vessels via beta activation and coronary dilation. Major parasympathetic effects are: increased GI motility; decreased sphincter tone; penile vasodilation leading to erection; skin vasodilation; increased glandular and GI secretion and coronary contraction. While blood flow is mostly increased by the ‘rest and digest’ parasympathetic system it is mostly decreased by the ‘fight or flight’ sympathetic system. In the brainstem (CNS) there are various control centres that mediate systemic homeostasis. The hypothalamus is involved in thermoregulation and osmoregulation; the respiratory centre and cardio inhibitory centre control pCO2-dependent ventilation rate and decrease HR respectively. The cardioacceleratory centre in the pons causes an increase in HR. The pneumotaxic centre, also in the brainstem, is involved in rhythmic inspiration inhibition to control amount of air inhaled. There is NANC transmission in the parasympathetic postganglionic fibre, off which comes a NANC fibre that releases VIP onto blood vessels. This hormone potentiates ACh action, causing vasodilation in arterioles and coronary arteries. In extreme conditions – fight or flight, balanced at rest with adjustment for exercise or temp change.