Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
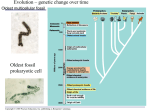
Respiration Processes Breathing (ventilation): air into and out of lungs External respiration: gas exchange between air and blood Internal respiration: gas exchange between blood and tissues Cellular respiration: oxygen use to produce ATP; carbon dioxide as waste Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Organs of the Respiratory system Nose Pharynx Larynx Trachea Bronchi Lungs – alveoli Figure 13.1 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Components of the Upper Respiratory Tract Nose, pharynx Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 10.2 Upper Respiratory Tract Functions: Passageway for respiration Receptors for smell Filters incoming air to block larger foreign material Moistens and warms incoming air Resonating chambers for voice Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Components of the Lower Respiratory Tract Functions: Larynx: maintains an open airway, routes food and air appropriately, assists in sound production Trachea: transports air to and from lungs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 10.3 Lower Respiratory Tract Functions: Bronchi: branch into lungs Lungs: transport air to alveoli for gas exchange Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Gas Exchange Between the Blood and Alveoli Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 10.8A Respiratory Membrane (Air-Blood Barrier) Thin squamous epithelial layer lining alveolar walls Pulmonary capillaries cover external surfaces of alveoli Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 13.6 Mechanics of Breathing (Pulmonary Ventilation) Completely mechanical process Depends on volume changes in the thoracic cavity, Which cause pressure changes, which lead to the flow of gases to equalize pressure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Inspiration - flow of air into lung Diaphragm and intercostal muscles contract size of thoracic cavity increases air is pulled into lungs due to decrease in intrapulmonary pressure Figure 13.7a Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Expiration– air leaving lung passive process; uses natural lung elasticity As muscles relax, air is pushed out of the lungs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Pressure Differences in the Thoracic Cavity Normal pressure within the pleural space is always negative (intrapleural pressure) Differences in lung and pleural space pressures keep lungs from collapsing Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Nonrespiratory Air Movements Can be caused by reflexes or voluntary actions Examples Cough and sneeze – clears lungs of debris Laughing Crying Yawn Hiccup Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Respiratory Volumes and Capacities Normal breathing moves about 500 ml of air with each breath (tidal volume [TV]) Many factors that affect respiratory capacity A person’s size Sex Age Physical condition Residual volume of air – after exhalation, about 1200 ml of air remains in the lungs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Respiratory Capacities Figure 13.9 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings External Respiration - gas exchange between air and blood Oxygen moves into the blood alveoli have more O2 than blood entering lungs O2 diffuses, binds to hemoglobin in RBC Carbon dioxide moves out of blood CO2 diffuses out of blood Carbonic acid shifts to CO2 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Gas Transport in the Blood Oxygen transport in the blood Inside RBCs attached to hemoglobin (oxyhemoglobin [HbO2]) O2 binds more readily at high pO2, neutral pH, and lower temperature Only 2% is dissolved in the plasma Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Gas Transport in the Blood Carbon dioxide Most CO2 is transported in the plasma as bicarbonate ion (HCO3–) 20% is carried inside RBCs on hemoglobin, but at different binding sites than used by O2 10% of CO2 is dissolved in plasma Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Internal Respiration Exchange of gases between blood and body cells Carbon dioxide diffuses out of tissue to blood Forms carbonic acid inside RBCs. Lowers pH and loosens O2 from hemoglobin Oxygen diffuses from blood into tissue Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Respiration Summary Figure 13.10 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Neural Regulation of Respiration Neural control located in medulla oblongata and pons Normal rate is 12–15 respirations per minute Hyperpnea is increased respiratory depth and vigor Figure 13.12 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Factors Influencing Respiratory Rate and Depth Chemical factors Carbon dioxide levels main regulatory chemical Increased CO2 increases respiration CO2 acts directly on the medulla oblongata via pH of cerebrospinal fluid Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Factors Influencing Respiratory Rate and Depth Chemical factors (continued) Oxygen levels O2 is detected by chemoreceptors in aorta and carotid artery Alert sent to medulla oblongata Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Factors Influencing Respiratory Rate and Depth Physical factors Increased body temperature Exercise Talking Coughing Volition (conscious control) Emotional factors Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Hyperventilation Hyperventilation - deep, rapid breathing Increases loss of CO2, so blood pH becomes more alkaline Can lead to apnea (no breathing), cyanosis, dizziness Treat by slowing respiration, rebreathing same air (use bag), or closing mouth, one nostril. Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Asthma hypersensitive bronchiole passages triggered by allergens (cat dander), exercise, viral infection, cold temperature Bronchioles close down, swell shut; produce more mucus Result: dyspnea, coughing, and wheezing Management includes monitoring vital capacity, steroids Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Respiratory Disorders: Chronic Obstructive Pulmonary Diseases (COPD) Ex. chronic bronchitis and emphysema Patients often with history of smoking Labored breathing (dyspnea) becomes progressively more severe Coughing, frequent pulmonary infections victims retain CO2, are hypoxic and have respiratory acidosis Ultimately, respiratory failure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Chronic Obstructive Pulmonary Disease (COPD) Figure 13.13 Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Lung Cancer Accounts for 1/3 of all cancer deaths in the United States Associated with smoking Smoke contains free radicals (nitrosamine) and other carcinogens that mutate DNA Lungs and other tissues exposed in smokers Metastasis common Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Sudden Infant Death syndrome (SIDS) Apparently healthy infant stops breathing and dies during sleep Some cases could be a problem of the neural respiratory control center One third of cases appear to be due to heart rhythm abnormalities Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings