Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
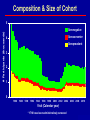
DOSSIER Web site: http://statepi.jhsph.edu/macs/macs.html Prepared by CAMACS Fax: 410-955-7587 The MACS is funded by the National Institute of Allergy and Infectious Diseases, with additional supplemental funding from the National Cancer Institute and the National Heart, Lung and Blood Institute. UO1-AI-35042, UL1-RR025005, UO1-AI-35043, UO1-AI-35039, UO1-AI-35040, UO1-AI-35041. May 2011 MACS Founding Principal Investigators Sites: Baltimore, MD - Frank Polk Chicago, IL - John Phair Los Angeles, CA - Roger Detels Pittsburgh, PA - Charles Rinaldo Data Coordinating Center Data Center – Alvaro Muñoz November 2004 MACS Sites and Principal Investigators Sites: • Baltimore, MD (J. Margolick) • Chicago, IL (J. Phair, S. Wolinsky) • Los Angeles, CA (R. Detels, O. Martinez• Maza) Pittsburgh (C. Rinaldo, L. Kingsley) Data Coordinating Center (CAMACS): • Baltimore, MD (L. Jacobson, A. Muñoz) November 2004 MACS Working Groups Behavioral (D. Ostrow) Hepatitis (C. Thio) Biomarker (C. Rinaldo) Malignancy/Pathology (O. Martinez-Maza) Cardiovacular (W. Post) Metabolic (L. Kingsley) Clinical (F. Palella) Neuropsychology (E. Miller) Core Laboratory (A. Butch) Renal (F. Palella) Data (L. Jacobson) Viral Immune Pathogenesis (J. Margolick) Genetics (S. Wolinsky) August 2010 Semiannual Visit Questionnaire / ACASI • Medical History, Health • Demographics Physical Examination / Lipodystrophy / Frailty Psychosocial • Quality of Life (SF36) • Depression (CESD) • Activities of Daily Living Labs • T-cells, HIV RNA, HBV & • Services, Behavior Medications: Antiretrovirals, OIspecific, Adherence HCV serology Lipids, liver and kidney function tests / anal cytology (IADL) Neuropsychological Screening Banked Specimens • Plasma, Serum, Cells • B-cell lines • PBMC pellets May 2009 Continuous Outcome Ascertainment Seroconversion Clinical Outcomes (medical records confirmation) • AIDS diagnoses • Non-AIDS diagnoses Cardiovascular disease Cerebrovascular disease Kidney disease Liver disease Lung infection, bacterima, septicemia Malignancies Neurologic • Mortality November 2004 CAMACS Planning and design of studies Coordination of data acquisition • Form development • Codebooks • Data transfer Standardization and data management • • Edits and updates Data security Data analysis, statistical computing and methodological research September 1995 MACS Database (as of May 2011) Publications (published & in press) 1,195 Participants 6,972 Person-Years 86,883 Variables 8,920 Repository aliquots 1,490,995 (plasma, serum, cells, urine) HIV+ HIV- Person-Visits 56,352 72,566 CD4 Measurements 51,798 57,808 HIV RNA Measurements 34,149 1,206 May 2011 MACS Subgroups of Particular Interest Long-term seropositive individuals with minimal declines in CD4 levels Seropositive individuals with rapid declines in CD4 levels Long-term survivors with low CD4 levels Seroconverters High-risk seronegatives Seropositives on treatment >55 years old Strengths of the MACS Comparison groups of similar risk • HIV-infected not receiving treatment • Uninfected persons Standardized, complete longitudinal data collected with uniform frequency, before and after treatment • Treatment information, behavior, physical examination, standard laboratory measurements • Facilitates implementation of new laboratory measurements Collect and reposit specimens • Facilitates nested studies • Allows retrospective testing of specimens as new laboratory • procedures become available Genetic data for predicting disease course/outcome and response to therapy Incidence* of Seroconversion in the MACS by Center Kingsley, Zhou, . . ., Muñoz - AJE 1991 (update) 60 Incidence Baltimore 50 Chicago 40 Pittsburgh Los Angeles 30 20 10 0 84 86 88 90 92 94 Calendar Time (years) * Incidence = # of seroconverters per 1,000 person-semesters September 1995 Number of Participants with Specimens Available* in the National Repository Relative to the Time of Seroconversion** Specimen Type Last Seronegative Visit First Seropositive Visit Plasma 465 508 Serum 487 486 Cells 450 443 * 2 or more tubes according to repository inventory as of 04/01/11 ** A total of 642 participants have a known seroconversion date May 2011 MACS Cohort 6972 Seroprevalent: 2884 (41.4%) Created Inactive 10/09 Seronegative: 4088 (58.6%) Seroconverter: 670 (16.4%) AIDS: 1611 (55.9%) Alive: 160 (9.9%) Active: 124 (77.5%) Dead: 1451 (90.1%) AIDS-Free: 1273 (44.1%) Alive: 1079 (84.8%) Active: 730 (67.7%) Dead: 194 (15.2%) 4/11 AIDS: 314 (46.9%) Alive: 54 (17.2%) Active: 41 (75.9%) Dead: 260 (82.8%) AIDS-Free: 356 (53.1%) Alive: 311 (87.4%) Active: 234 (75.2%) Dead: 45 (12.6%) Seronegative: 3418 (83.6%) Not Censored: Censored:* 1708 1710 (50.0%) (50.0%) Alive: 1578 (92.3%) Dead: 132 (7.7%) Active: 1182 (74.9%) * HIV seronegative participants were administratively censored from the MACS in 1993 May 2011 Composition & Size of Cohort # Participants (thousands) 5 Seronegative Seroconverter 4 Seroprevalent 3 2 1 0 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 Visit (Calendar year) * 1710 have been administratively censored May 2011 Examples of Research Studies Progression of HIV-1 Infection Prior to Potent Antiretroviral Therapy Muñoz, Xu. Stat Med 1996; Enger et al. JAMA 1996; Jacobson et al. AJE 1993 (update) 1.0 Origin SC CD4# 200 AIDS Proportion 0.8 Event AIDS DEATH DEATH 1199/2137 1093/1313 1213/1620 0.6 1.3 2.7 8.9 median 0.4 0.2 5.3 0.0 0 5 10.3 Time in Years 10 5 percent 15 October 1998 Likelihood of Developing AIDS in Three, Six and Nine Years Mellors, Muñoz,…, Rinaldo. Ann Int Med 1997 Li, Buechner,…, Muñoz. Am Statistician 2003 0 4 2 2 10 2 17 3 17 2 8 8 1500-7K 16 40 >7K-50K HIV-RNA (copies/ml) RT-PCR 40 >20K-50K >55K 33 14 37 37 >750 33 #1500 501-750 48 64 86 17 16 8 #1500 10 37 1500-7K 351-500 201-350 HIV-RNA (copies/ml) RT-PCR #200 CD4+ T-Lymphocyte (cells/mm3) 55 55 73 >7K-50K 73 >20K-50K >55K 37 >750 67 501-750 78 351-500 89 98 67 201-350 #200 CD4+ T-Lymphocyte (cells/mm3) 4 22 35 35 35 40 60 60 #1500 60 1500-7K >7K-50K 76 76 86 86 62 >750 76 94 93 76 501-750 351-500 HIV-RNA >20K-50K 201-350 100 (copies/ml) CD4+ T-Lymphocyte #200 >55K (cells/mm3) RT-PCR 17 Predictors of Short- and Long-Term Survival after Reaching <50 CD4+ T-cells/mm3 (1) Marker T-cell reserve Survival >18 months <6 months (N=26) P (N=11) HLA-DR- CD38(resting) CD4 % 36 (8-49) 20 (4-43) .02 HLA-DR- CD38(resting) CD8 % 22 (5-51) 13 (2-29) .01 Predictors of Short- and Long-Term Survival after Reaching <50 CD4+ T-cells/mm3 (2) Giorgi et al., JID 1999; 179:859-870 Marker T-cell activation Survival >18 months <6 months (N=26) (N=11) P CD4 T-cell expression of CD38 (RFI) 87 (28-466) 221 (59-487) .002 CD8 T-cell expression of CD38 (RFI) 190 (81-638) 411 (163-661) .001 HLA-DR+ CD38CD8 % 7 (0.7-18) 1.9 (0.4-8) .002 Plasma HIV-1 copies/mL 105.2 (104.5-106.3) 105.6 (104.9-106.1) .02 Interpretation: Activation is a more important determinant of survival at low CD4+ levels than viral load Detels/Imagawa Study, 1989 (1) Methods: Isolation studies (unique protocol) of 133 repeatedly exposed MSM Results: HIV isolations from 31; subsequently, four seroconverted 11-17 months after positive isolation 27 isolation/PCR-positive MSM persistently antibody-negative 36+ months Interpretation: The 27 men cleared the virus Imagawa DT, et al. Human immunodeficiency virus type 1 infection in homosexual men who remain seronegative for prolonged periods. N Engl J Med 1989; 320(22):1458-1462. Resistant vs Susceptible MSM Detels, 1994 Resistant MSM: 100 persistently HIVnegative highly exposed MSM Susceptible MSM: 77 low-risk seronegatives Results: Increased levels of neutrophils and CD8+ cells in resistant men Interpretation: CD8 cells may modulate outcome of HIV exposure Detels R, et al. Resistance to HIV-1 infection. J Acquir Immune Defic Syndr 1994; 7:1263-1269. Genetic and Immunologic Studies of Resistant MSM - Detels, 1996 Immunologic Study 13 “resistant” MSM 27 seroconverters Results: Median percentage of CD25+/CD8+ activated cells higher in resistant men Genetic Study 23 resistant men 137 low-risk seroconverters Results: Significantly higher levels of TAP 1.4 and TAP 1.4/2.3 genes in resistant men Interpretation: Genetic factors (MHC transport?) are associated with resistance to infection Detels R, et al. Persistently seronegative men from whom HIV-1 has been isolated are genetically and immunologically distinct. Immunol Lett 1996; 51:29-33. CCR5 Confers Protection Methods/Results: 111 resistant, 4.5% CCR5 homozygous 614 seropositive, 0% CCR5 homozygous Interpretation: 100% absence of CCR5 receptor on CD4 cells confers 100% protection Zimmerman PA, et al. Inherited resistance to HIV-1 conferred by an inactivating mutation in CC chemokine receptor 5: studies in populations with contrasting clinical phenotypes, defined racial background, and quantified risk. Mol Med 1997; 3(1):23-36. AIDS-Free Time by Calendar Detels, Muñoz, . . ., Phair - JAMA 1998 (update) 100 90 Percent AIDS-Free 80 70 60 50 40 30 20 10 Calendar N AIDS RH 86.0 to 89.5 89.5 to 93.0 93.0 to 96.5 96.5 to 99.5 341 427 378 264 36 91 100 20 1.48 1 0.92 0.30 4 5 (p-value) (0.119) (0.626) (<.001) RT (p-value) 1 1.03 2.11 (0.690) (<.001) 0 0 1 2 3 6 7 8 9 10 11 12 13 14 Years since Seroconversion Interpretation: HAART delays onset of AIDS May 2000 Effect of HLA-B Alleles on AIDS Progression (N=1,089) Gao, Bashirova, …, Carrington. Nat Med 2005 B*57 B*35Px 1.0 1.0 0.9 0.9 0.8 0.7 0.6 RH=0.43 p<0.0001 0.5 0.4 0.3 0.2 0.1 RH=1.63 p<0.0001 RH=0.71 P=0.03 Fraction AIDS 1987 free Fraction AIDS 1993 free B*27 others 0.8 0.7 0.6 0.5 RH=0.4 9 P=0.001 0.4 0.3 RH=0.5 P=0.003 0.2 RH=1.92 p<0.0001 0.1 0 0 0 2 4 6 8 10 12 14 16 18 Time since seroconversion (year) 0 2 4 6 8 10 12 14 16 18 20 Time since seroconversion (year) Interpretation: HLA-B allele influences progression May 2006 Kaplan-Meier Survival Curves for Genotypes of SNP rs17762192, Representing a Haplotype Located 36kb Upstream of PROX1 and Chromosome 1, Showing Strong Associations with Differing Rates of Progression to Clinical AIDS Herbeck, Gottlieb, … Mullins. J Infect Dis 2010 A. Replication cohort (ALIVE, MACS, MHCS, SFCC, individuals genotyped by Steve O’Brien B. Combined analysis of replication and discovery cohorts (156 MACS individuals enriched with rapid progressors and long-term non-progressors May 2010 Time to AIDS Following HAART According to Selected Genotypings Hendrickson, Jacobson, . . ., O’Brien - JAIDS 2008 Interpretation: CCR5-∆32 + SDF1-3’UTR delay onset of AIDS May 2009 Association between CD4+ T-cell Count (cells/µℓ) and Prevalence of Carotid Lesions among Participants in Men (MACS) and Women (WIHS) Kaplan, Kingsley, . . ., Hodis - AIDS 2008 3.5 - - 3.0 Prevalence ratio 2.5 - 2.0 - 1.5 - - 1.0 - - - - - 0.5 HIV- HIV+ HIV+ CD4>500 350-500 200-349 N=325 N=303 N=147 N=100 HIV+ HIV+ <200 N=50 Men HIV- HIV+ HIV+ CD4>500 350-500 200-349 N=496 N=487 N=269 N=288 HIV+ HIV+ <200 N=187 Women Interpretation: Decreasing CD4+ level is associated with increasing CVD risk May 2009 Premature Aging of T cells Is Associated With HIV-1 Percentages of CD57+ cells within the CD4+ or CD8+ T cells Interpretation: HIV-1 infection is associated with shift toward aged conformation of Tcells; i.e., HIV induces accelerated aging of T-lymphocytes Cao et al., JAIDS 50:142, 2009 Percentages of CD8+ T-cell subsets defined by expression patterns of CD28 and CD57 An Evolving Scientific Agenda (partial) (1) 1985: HIV virology 1986: Neuropsychology 1987: Biostatistical methodology and therapeutics 1989: Cancer 1993: Health care utilization 1999: Metabolic complications An Evolving Scientific Agenda (partial) (2) 2001: Hepatitis 2003: Cardiovascular disease 2005: Aging and sleep 2008: Renal complications and hearing and balance 2010: Genetic determinants of immune response and response to treatment 2010: Premature aging of immune function Keys to Success 1. Commitment of the participants!!! 2. Dedication of the staff 3. Standardization and quality control of data collection, laboratory procedures, and record keeping 4. Decision to establish a repository of specimens 5. Reaching out to other investigators with essential expertise 6. Staying on the “cutting edge” 7. Consistent funding 8. Foresight and competence of original and subsequent investigators