Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
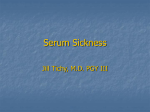
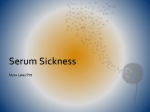
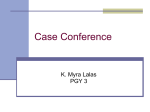
Serum Sickness Definition A clinical syndrome that results from the injection of heterologous foreign protein or serum that leads to deposition of antibody-antigen complexes in the blood vessel wall Classic example of a systemic Gell and Coombs type III immunological reaction Serum sickness-like reactions are secondary to nonprotein drugs but often cause indistinguishable reactions History First described by Schick and VonPirquet in 1905 Horse anti-diptheria antitoxin Reproducible syndrome in patients Fever, malaise, rash, tender lymphadenopathy, leukopenia, arthralgias, albuminuria and edema Occurred 8-13 days after first injection of horse sera Incidence of symptoms related to amount of sera given 5-15 cc of anti-toxin resulted in 5-10% incidence of serum sickness 100-200 cc of anti-toxin resulted in >85% incidence Incidence Decreasing incidence of classic serum sickness Vaccination programs Refined horse serum antitoxins Current use of human antiserums Rabies Tetanus Non-protein drugs now most common causes Incidence Directly related to amount and type of foreign serum injected In one study, 10% patients receiving 10ml tetanus antitoxin developed serum sickness, whereas, all of those receiving 80ml developed serum sickness Anti-rabies serum produces higher incidence (~16%) versus tetanus antitoxin (2.5-5%) Current Use of Foreign Serum Botulism Diphtheria Tetanus – equine, human antitoxin Snake bites (rattlesnakes,copper heads,cottonmouth) Black widow/Latrodectus species Scorpion Antilymphocyte antibody Digoxin immune FAB (Digibind) Other Agents Causing Serum Sickness Allopurinol Anti-thymocyte globulin Arsenicals derivatives Barbituates Bupropion Captopril Carbamazepine Cephalosporins Cholecystographic RCM Ciprofloxin Dextran Fluoxetine Furazolidone Gold Salts Griseofulvin Halothane Hydralazine Iodides Indomethacin Infuenza Vaccine Itraconazole Methyldopa Other Agents Causing Serum Sickness Mercurial derivatives Metronidazole NSAIDs Penicillamine Penicillins Phenylbutazone Phenytoin Piperazine Procainamide Propranolol Rifampin Quinidine Streptokinase Sulindac Sulfonamides Tetracycline Thiouracils Still more causes Also… Allergen extracts Blood products Hormones Vaccines Infectious agents Monoclonal antibodies Hymenoptera stings Tick bites What is Going on? Foreign antigen introduced Antibodies develop and can form complexes with the antigen Depending on the size and amount of complexes, they may deposit on vascular wall Smaller vessels more common Leads to vasculitis, nephritis, and arthritis Fixation and activation of complement What is Going on? Increase in Anaphylatoxins like C3a and C5a Causes mast cells to degranulate Leads to PMNs influx to area of inflammation Endothelial cells increase expression of adhesion molecules (like ICAM) Proinflammatory cytokines are released by monocytes and macrophages Proteolytic enzymes are released and mediate damage (and symptoms) Mast Cell Mediators Preformed mediators Histamine Proteases Tryptase Acid hydrolases Proteoglycans Cytokines (TNF-α, IL-4) Newly formed mediators Prostaglandins Leukotrienes Thromboxanes Platelet activating factor What is Going on? Increase in Anaphylatoxins like C3a and C5a Causes mast cells to degranulate Leads to PMNs influx to area of inflammation Endothelial cells increase expression of adhesion molecules (like ICAM) Proinflammatory cytokines are released by monocytes and macrophages Proteolytic enzymes are released and mediate damage (and symptoms) Why Does the Body do This? Body’s way of dealing with some insults by complexing them before they can elicit their damage These complexes then cleared by RE system Serum sickness is a systemic process whose symptoms are determined by where immune complexes are deposited There is localized serum sickness reaction called Arthus reaction Other human immune-complex diseases SLE, PAN, PSGN Why Continued… Larger complexes are cleared more readily, smaller complexes more apt to deposit Complexes with cationic charge may bind negative BM more readily IgG more likely culprit in forming the complexes that are seen in serum sickness Amount and size of complexes based on the amount of antigen versus antibody present in system at the time (Zone of Equivalence) • Formation of small antigenantibody complexes which are soluble and poorly cleared • Complex deposition may be exacerbated by increased vascular permeability caused by mast cell activation via FcgammaRIII (CD16) • The deposited immune complexes trigger neutrophils to discharge their granule contents with consequent damage to the surrounding endothelium and basement membranes Nick Holmes; Cambridge univerisity Department of Pathology -Immunology division •The complexes may be deposited in a variety of sites such as skin, kidney and joints Radio-labeled bovine serum albumin is injected intravenously into normal rabbits at day 0, and sequence of immunologic events is followed. At about day 8, immune complexes are formed, complement levels fall, and rabbits become ill. Complement Antigen Antibodies Complexes Zone of Equivalence Lawley TJ, Frank MM In Parker C, editor: Clinical immunology, Philadelphia, 1980, WB Saunders Clinical Symptoms Occur 6-21 days after administration of foreign antigen Typically 7-14 days Accelerated symptoms within 2-4 days in patients previously sensitized Often pain, pruritis, erythema and swelling at injection site Most cases resolve in a few days to a couple of weeks Clinical Symptoms Fever Mild to significant 5-14 days after exposure Lymphadenopathy Can be regional (at site) or generalized Arthralgias More common in large joints like knees Metacarpal and TMJ also seen Pain often out of proportion Clinical Symptoms Arthritis less common Some patients may feel chest pain or shortness of breath Edema may occur (especially face and neck) Some patients may have visceral involvement such as hepatomegaly Cutaneous Eruptions Present in 95% Urticaria - mediated by IgE and/or complement Morbilliform eruption Maculopapular exanthem Erythema multiforme Purpura Angioedema, especially of face and neck Skin rash in serum sickness • Received equine anti- thymocyte globulin therapy 12 days prior to rash • Morbilliform and urticarial rash began on the torso and back, then spread to the extremities • The rash was accompanied by circulating immune complexes Cutaneous Eruptions Characteristic serpiginous erythematous, purpuric eruption at the junction of palmar and plantar skin and the dorsum of the hands and feet Reported in 75% of patients receiving antithymocyte globulin in one study Serpiginous Erythematous (purpuric eruption at the junction of palmar and plantar skin) Other Manifestations Generalized vasculitis Peripheral neuritis Brachial Plexus most common Guillain-Barre rare Glomerulonephritis Labs May see proteinuria or hematuria May see a leukocytosis or leukopenia May have eosinophilia May have elevated ESR Decreased complement (C3 and C4), increased C3a The Complement Pathways Lectin pathway Kuby, 336 Diagnosis Typical symptom complex in a patient given foreign protein or drug within the appropriate time interval Symptoms have not lasted longer than one month No single laboratory test is confirmatory Treatment Stop offending agent -should lead to resolution of the signs and diagnosis within a period of days to a few weeks Symptoms are usually mild and spontaneously resolve in a few days or weeks with symptomatic therapy Antihistamines and NSAID’s relieve the pruritis and pain Treatment of Severe Serum Sickness Corticosteroids Administered and tapered over 10-14 days Shorter courses are associated with relapses Relapses are more difficult to alleviate Prophylaxis Incidence of serum sickness may be reduced by pretreatment with antihistamines Negates the effect of vasoactive amines Decreases vascular permeability Reduces passive deposition of immune complexes