Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
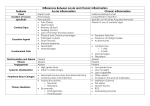
Inflammation Dr.ROOPA Premed 3 Pathophysiology Introduction: “Inflame” – to set fire. “Inflammation is a reaction of a tissue and its microcirculation to a pathogenic insult. It is characterized by the generation of inflammatory mediators and movement of fluid & leukocytes from the blood into extravascular tissues.” “dynamic response of vascularised tissue to injury.” Is a protective response. Serves to bring defense & healing mechanisms to the site of injury. 2 Naming of inflammatory diseases: [prefix] + ‘itis’ (exceptions exist) crohn’s disease 3 Types of Inflammation Acute Chronic Acute Inflammation Acute inflammation is a rapid response to an injurious agent that serves to deliver mediators of host defense—leukocytes and plasma proteins—to the site of injury. Acute inflammation has three major components: (1) alterations in vascular caliber that lead to an increase in blood flow; (2) structural changes in the microvasculature that permit plasma proteins and leukocytes to leave the circulation; and (3) emigration of the leukocytes from the microcirculation, their accumulation in the focus of injury, and their activation to eliminate the offending agent Acute inflammatory reactions are triggered by a variety of stimuli: • Infections (bacterial, viral, parasitic) and microbial toxins • Trauma (blunt and penetrating) • Physical and chemical agents (thermal injury, e.g., burns or frostbite; irradiation; some environmental chemicals) • Tissue necrosis (from any cause) • Foreign bodies (splinters, dirt, sutures) • Immune reactions (also called hypersensitivity reactions) Acute Vs Chronic Flush, Flare & Wheal Acute inflammatory cells - Neutrophils Vascular damage More exudation Little or no fibrosis Little signs Fibrosis, Chronic inflammatory cells – Lymphocytes Neo-vascularisation No/less exudation Prominent fibrosis 7 Table 5–1. Differences between Acute and Chronic Inflammation. Acute Chronic Duration Short (days) Long (weeks to months) Onset Acute Insidious Specificity Nonspecific Specific (where immune response is activated) Inflammatory cells Neutrophils, macrophages Lymphocytes, plasma cells, macrophages, fibroblasts Vascular changes Active vasodilation, increased permeability New vessel formation (granulation tissue) Fluid exudation and edema + – Cardinal clinical signs (redness, heat, swelling, pain) + – Tissue necrosis + (ongoing) – (Usually) + (Suppurative and necrotizing inflammation) Fibrosis (collagen deposition) – + Operative host responses Plasma factors: complement, immunoglobulins, properdin, etc; neutrophils, nonimmune phagocytosis Immune response, phagocytosis, repair Systemic manifestations Fever, often high Low–grade fever, weight loss, anemia Changes in peripheral blood Neutrophil leukocytosis; lymphocytosis (in viral infections) Frequently none; variable leukocyte changes, increased plasma immunoglobulin Cardinal Signs of Inflammation Rubor : Redness – Hyperaemia. Calor : Warm – Hyperaemia. Dolor : Pain – Nerve, Chemical med. Tumor: Swelling – Exudation Loss of Function: Eg. 10 The 5 Cardinal Signs of Heat Redness Swelling Pain Loss Of Func. 11 Inflammation - Mechanism 1. Vaso dilatation 2. Exudation - Edema 3. Emigration of cells 4. Chemotaxis 13 Mechanism of Inflammation: 14 Leukocyte cellular events Leukocytes leave the vasculature routinely through the following sequence of events: – Margination and rolling – Adhesion and transmigration – Chemotaxis and activation They are then free to participate in: – Phagocytosis and degranulation – Leukocyte-induced tissue injury 15 PRINCIPAL CELL EFFECTORS 1st 24 hours: NEUTROPHILS Bacterial infections, infarction Come from the bone marrow reserve pool Band neutrophils: less mature cells Neutrophils -- the key cell type of the acute inflammatory response 17 2nd-3rd day: neutrophils are replaced by monocytes-macrophages Tuberculosis, salmonellosis Eosinophils Allergic reactions Parasitic infections Hodgkin lymphoma Mast cells and basophils Chronic myelogenous leukemia Myeloproliferative diseases histamine Cellular response of leukocytes Emigration Margination Pavementing Rolling/Tumbling Adhesion Transmigration Chemotaxis Phagocytosis Opsonization Intracellular microbial killing Oxygen-dependent Oxygen-independent MARGINATION THE ENDOTHELIAL CELLS ARE ACTIVATED, ATTRACT THE SURFACE GLYCOPROTEINS ON NEUTROPHILS DIAPEDESIS INSINUATION OF THE NEUTROPHILS THRU THE ENDOTHELIAL CELLS BASEMENT MEMBRANE EXTRAVASCULAR TISSUES CHEMOTAXIS NEUTROPHIL DIRECT ITS MIGRATION TOWARDS THE CHEMOATTRACTANT PHAGOCYTOSIS FORMATION OF PHAGOSOME LYSOSOME PHAGOLYSOSOME Intracellular microbial killing: Oxygen-dependent killing is the MOST important microbial process Phagocytosis activates HMP shunt oxidative burst suppplies electrons to NADPH oxidase superoxide anion Hydrogen peroxide Hydrogen peroxide Oxides microbial proteins and disrupts cell walls Myeloperoxidase-halide system of bacterial killing After killing and eliminating the microbes, the activated leukocytes play other functions 1.Macrophages produce GF(growth factor) that stimulate endothelial cell proliferation and fibroblasts. 2.Synthesis of collagen 3,Aids in the process of repair. DEGRANULATION THE TOXIC SUBSTANCES MAY CAUSE LOSS OF FUNCTION (FUNCTIO LAESA) INCREASED BLOOD FLOW DUE TO RELAXATION OF THE TERMINAL ARTERIOLES RUBOR AND CALOR CONTRACTION OF CAPILLARY ENDOTHELIAL CELLS INCREASED VASCULAR PERMEABILITY SWELLING TUMOR MILDEST: EXTRAVASATION OF WATER, LOW MOLECULAR WEIGHT PROTEINS MODERATE: + HMW(high molecular weight) PROTEINS SEVERE: + BLOOD CELLS MEDIATORS OF ACUTE INFLAMMATION Exogenous: microbial products Endogenous: 1. vasoactive amines histamine serotonin 2. Arachidonic acid metabolites cyclooxygenase pathway lipooxygenase pathway 3. Cytokines 4. Kinin system 5. Complement system Histamine increase capillary permeability contracts postcapillary venules Source: basophils, mast cells,platelets Stimuli: binding of IgE binding of C3a and C5a:”anaphylotoxins” heat, cold Interleukin-1 Serotonin 5-hydroxytryptamine Action: similar to histamine Source: platelets Arachidonic acid metabolites Cyclooxygenase pathway Enzymes:COX-1,COX-2 Products: 1. Platelet TxA2 -vasoconstrictor,platelet aggregator 2. Endothelial prostacyclin -vasodilator,inhibits platelet aggregation Lipooxygenase pathway Products: hydroperoxyeicosatetraen oic acid (HPETE) 5-HPETE -leukotrienes Important leukotrienes LTB4: chemotactic for neutrophils LTC4,LTD4,LTE4 “slow reacting substance of anaphylaxis” vasocontriction bronchospasm (bronchcontriction) increase capillary permeability Cytokines Soluble proteins Secreted by numerous cells(monocytes-macrphages) Act as “effector molecules” IL-1 and TNF “acute phase response” Fever, increase WBC: systemic Synthesis of C-reactive proteins, complement components, fibrinogen, prothrombin Synthesis of adhesion molecules Neutrophil degranulation Kinin system Formed during active secretion in sweat glands, salivary glands, pancreas, kidneys End product: bradykinin Actions: vascular permeability arteriolar dilation pain Complement system 20 Plasma proteins HEPATOCYTES,MACROPHAGES, GIT CELLS Action: cell lysis COMPLEMENT CASCADE classical pathway alternative pathway OPSONIZE BACTERIA ACTIVATE PMN, MACROPHAGES REGULATES AB RESPONSE CLEARS AWAY IMMUNE COMPLEXES INFLAMMATION, TISSUE DAMAGE ANAPHYLAXIS MAC Classical pathway vs alternative pathway Starts with C1 + antigen-antibody Bacterial surface activates the pathway Ends with the membrane attack complex Works in the absence of antibodies Less efficient C3b: opsonin C3a and C5a: anaphylotoxins C5b-C9: “MAC” membrane attack complex Inflammation Outcome Fibrosis/Scar Resolution Injury Acute Inflammation Chronic Inflammation Abscess Ulcer Fistula Sinus 54 ABSCESS Cavity filled with pus Pus: neutrophils, monocytes and cellular debris Fibrous wall Inaccessible to circulation Bacterial infections, especially staphylococci Ulcer Involves epithelial surfaces Loss of surface epithelium Fistula Abnormal communication between 2 organs or between an organ and a surface Scar Final result of tissue destruction Distortion of structure Altered function Patterns of chronic inflammation Chronic nonspecific inflammation Granulomatous inflammation Chronic nonspecific inflammation Proliferation of fibroblasts and new vessels Increased macrophages, lymphocytes, plasma cells Macrophage+antigen B lymphocyte activation antibody-producing plasma cells Scarring and distortion of tissue architecture Most characteristic: CASEOUS NECROSIS Multinucleated giant cells TB, fungal infections, Syphyllis, cat-scratch fever, foreign bodies