Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
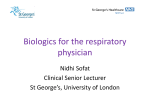
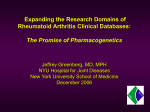
Asthma and Anti-TNF-α Therapeutics Jessie Scott MCB 5255 Overview Asthma TNF-α Anti-TNF-α Therapies Paper 1 Paper 2 Future Directions Specific Aim Asthma Allergic respiratory disease with complex cytokine interactions, involving airway inflammation, mucus hypersecretion, reduced breathing ability, and airway remodeling in response to allergens 2 types: Mild-Moderate asthma: involves Th2 lymphocytes, eosinophils, and high levels of IgE. Treatable by corticosteroids Severe Refractory Asthma: involves Th1 lymphocytes, Th17 lymphocytes, neutrophils and some eosinophils, and TNF-α Not treatable by corticosteroids Heterogeneous phenotypes Need to distinguish between these two types for appropriate treatment Hansbro et al. 2011 TNF-α and asthma Effects of TNF-α on the respiratory system It causes the recruitment of pro-inflammatory cells and affects airway remodeling – typical asthma symptoms Inhaled recombinant human TNF-α has been demonstrated to cause a decrease in forced expiratory volume (FEV) and increased neutrophil and eosinophil recruitment Brightling et al. 2008 Effect of control or tumour necrosis factor alpha (TNFα) inhalation upon log PC20 expressed as percentage of the baseline value after 24 and 48 hours. Thomas P S , and Heywood G Thorax 2002;57:774-778 Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved. (A) Effect of control (open bars) or tumour necrosis factor alpha (TNFα, shaded bars) inhalation on change in percentage neutrophils from baseline for the 3 days of the study (ANOVA, p<0.01; post hoc Bonferroni corrected t test, *p<0.05,**p<0.02). Thomas P S , and Heywood G Thorax 2002;57:774-778 Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved. TNF-α Starts as transmembrane TNF (tmTNF) Cleaved by TNF-α converting enzyme (TACE), then it becomes soluble TNF (solTNF) Binds to TNFR1 or TNFR2, stimulates transcription of proinflammatory genes Extracellular domains of TNFR can be cleaved to regulate TNF-α levels http://www.ajpcr.com/Vol4Suppl1/551.pdf TNF-α Signaling TNF- α binds to TNFR1 or TNFR2 TNFR1 is expressed on all cells and primarily binds solTNF TNFR2 is expressed primarily on immune cells and binds both solTNF and tmTNF TNFR1 signaling can lead to apoptosis activation through the caspase 8 pathway TNFR1 and TNFR2 both lead to the expression of inflammatory genes and cell survival tmTNF tmTNF has been implicated in tumor immune evasion in some cases tmTNF binds to TNFR2, these receptors are involved in Treg functions and myeloid-derived suppressor cell (MDSC) accumulation – these cells allow for immune evasion of tumor cells (Hu et al. 2013) tmTNF was found to increase the suppressive effects of MDSC while solTNF did not This increase was stopped by TNFR2 inhibition A mutant non-cleavable tmTNF also led to increased tumorigenesis in cell culture Another study found that breast cancer cells displayed high levels of tmTNF (Yu et al. 2013) A monoclonal antibody to tmTNF demonstrated tumor suppression and even regression in a mouse model bearing breast cancer tumors http://www.jleukbio.org/content/88/5/827/F1.large.jpg Anti-TNF-α Treatments Etanercept – human fusion protein made of TNF-αR2 and the Fc region of IgG1 Subcutaneous injection Non-selective for tmTNF or solTNF Doesn’t activate complement system (Brightling et al. 2008) Infliximab – chimeric monoclonal antibody made up of human Ig constant region, 2 mouse variable regions to TNF-α Can trigger complement system Non-selective for tmTNF or solTNF DN-TNF – dominant negative TNF, mutated TNF that forms heterotrimers with native TNF to decrease its binding efficiency to TNFRs http://media.pharmacologycorner.com/wp-content/uploads/2009/05/tnfmoa7.gif Paper 1 Goal: To determine the differences (if any) between anti-TNF therapy and corticosteroid therapy on airway remodeling in asthma. Conducted comparisons and looked at statistical significance between etanercept and each other experimental situation (untreated asthma, healthy control, and dexamethasone) for different tissue remodeling factors. Figure 1 This displays how the experimental model for asthma was generated Mice were treated once a week with IP OVA for 2 weeks They were then treated with aerosolized OVA for 30min/day for 3 days each week for 10 weeks During the last two weeks, mice also received etanercept, dexamethasone, or saline IP Mice were then sacrificed and airway epithelia was examined Figure 2 Data displaying the basement membrane thickness, smooth muscle thickness, and epithelial thickness of airways from asthmatic mice that were untreated, or treated with steroids or etanercept. Etanercept demonstrates reduced basement membrane thickness and epithelial thickness compared to the untreated asthma. The steroid demonstrates decreased basement membrane, smooth muscle, and epithelial thickness compared to the untreated asthma Conclusion: All data is statistically significant Etanercept vs Healthy Control Conclusion: Etanercept treatment could not reduce subepithelial muscle and basement membrane thickness compared to healthy control. Etanercept could revert remodeling so that epithelial layer thickness and goblet cell number were not significantly different compared to healthy control. Etanercept vs Untreated Asthma Conclusion: Etanercept treatment significantly reduced: epithelial and basement membrane thickness goblet cell number Mast cell number Etanercept could not reduce subepithelial muscle layer thickness Etanercept vs Dexamethasone Conclusion: No statistical significant difference between treatments on: epithelial thickness basement membrane thickness mast cell number However, steroid treatment was better for decreasing subepithelial muscle layer thickness Summary of Paper 1 Anti-TNF-α treatment with etanercept led to a decrease in: epithelial and basement membrane thickening Mast cell number Goblet cell number (better than steroid treatment) It could not decrease subepithelial muscle layer thickness significantly like dexamethasone could; it is comparable to dexamethasone in all other measures Similarities may be due to steroid-caused reduction in TNF-α levels Paper 2 Goal: To determine whether inflammation is mediated by solTNF or tmTNF and investigate if dominant-negative TNF (DN-TNF) therapy can reduce TNF inflammation Figure 1 Used TNF knockout mice (no tm or solTNF) and tmTNF knock in mice to study effects of solTNF and tmTNF on eosinophil and macrophage recruitment, and lung activity of eosinophil peroxidase Conclusion: solTNF mediates allergic lung inflammation symptoms: eosinophil and macrophage recruitment and EPO activity Figure 2 Stimulated asthma with ovalbumin immunization and challenge in Balb/c mice Treated mice with etanercept, a nonselective anti-TNF treatment Used XENP1595 and XENP346 as dominant negative control of soluble TNF (DN-TNF) DN-TNF worked just as well as etanercept for reducing eosinophil recruitment and activity DN-TNF worked better than etanercept in reducing lymphocyte recruitment Conclusion: soluble TNF mediates inflammatory lung response, these side effects are controlled well by DN-TNF therapy Figure 3 http://www.frontiersin.org/files/Articles/30094/fphar-03-00156-r4/image_m/fphar-03-00156-g005.jpg Lung resistance and compliance was measured by plethysmography Mice treated with etanercept or DN-TNF had better compliance and less resistance than mice that were untreated Conclusion: etanercept and DN-TNF both increase lung compliance, therefore solTNF is what mediates airway resistance Figure 4 Treated with etanercept or DN-TNF at time of challenge didn’t yield as good results as treatment at the same time as immunization and challenge (see previous figures) Conclusion: treatment at time of immunization and challenge worked better, but etanercept and DN-TNF were both able to reduce eosinophil recruitment Figure 5: H&E Staining H&E staining demonstrating areas of eosinophil infiltration Conclusion: Anti-TNF treatments reduced eosinophil infiltration. Figure 5: PAS Staining PAS staining demonstrating areas of goblet cell hyperplasia and hypersecretion of mucus Conclusion: Anti-TNF decreased goblet cell hyperplasia and mucus secretion the most. Figure 6 Inflammatory cytokines and IgE from BAL samples were measured by ELISA. Conclusion: Anti-TNF treatments reduced inflammatory cytokines and IgE levels. Paper 2 Summary Soluble TNF mediates the inflammatory effects of TNF Regulation of solTNF through DN-TNF therapy can reduce asthma symptoms such as eosinophil recruitment, EPO activity, macrophage recruitment, goblet cell hyperplasia, mucus secretion, and lung compliance. Etanercept and other non-selective anti-TNF therapies are not recommended for asthma treatment because of the negative side effects from immunosuppression However, DN-TNF may be an effective asthma therapy because it preserves the innate immune activity of tmTNF while reducing asthma symptoms Future Directions A suitable treatment for Severe Refractory Asthma still does not exist, etanercept and infliximab are useful in some cases, but not all The risk-benefit ratio for using non-selective anti-TNF therapies is not ideal Mediating soluble TNF decreases the inflammation, but does not affect susceptibility to infection – DN-TNF may be the solution to severe refractory asthma treatment Specific Aim: Stimulate tumor formation in mice using ultraviolet irradiation on TNFknockout mice, tmTNF knock in mice, and while treating wild-type mice with DN-TNF or etanercept to observe any differences in the rate of tumor formation. If the tmTNF knock in mice and the DN-TNF treated mice form less tumors, then tumor suppression is mediated by tmTNF. This will help clarify whether DN-TNF could be used as a safe and effective asthma treatment Thank you! Works Cited Brightling C, Berry M, and Amrani Y. (2008). Targeting TNF-alpha: a novel therapeutic approach for asthma. The Journal of allergy and clinical immunology 121:5-10. Hansbro PM, Kaiko GE, Foster PS. (2011). Cytokine/anti-cytokine therapy – novel treatments for asthma? British Journal of Pharmacology 163:81-95. Hu X, Li B, Li X, Zhao X, Wan L, Lin G, Yu M, Wang J, Jiang X, Feng W, Qin Z, Yin B, Li Z. (2014). Transmembrane TNF-a promotes suppressive activities of myeloid-derived suppressor cells via TNFR2. Journal of Immunology 192:1320-1331. Maillet I, Schnyder-Candrian S, Couillin I, Quesniaux VFJ, Erard F, Moser R, Fleury S, Kanda A, Dombrowicz D, Szymkowski DE, Ryffel B. (2011). Allergic lung inflammation is mediated by soluble tumor necrosis factor (TNF) and attenuated by dominant-negative TNF biologics. American Journal of Respiratory Cell and Molecular Biology 45: 731-739. Thomas PS and Heywood G. (2002). Effects of inhaled tumour necrosis factor alpha in subjects with mild asthma. Thorax 57:774-778. Yilmaz O, Karaman M, Bagriyanik HA, Firinci F, Kiray M, Turkeli A, Karaman O, Yuksel H. (2013). Comparison of TNF antagonism by etanercept and dexamethasone on airway epithelium and remodeling in an experimental model of asthma. International Immunopharmacology 17: 768773. Yu M, Zhou X, Niu L, Lin G, Huang J, Zhou W, Gan H, Wang J, Yin B, Li Z. (2013). Targeting transmembrane TNF-a suppresses breast cancer growth. Cancer Research 73:4061-4074.