Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prepared by :
Mr. Ahmad Abu-Rahma
Mr. Ayman El-Ghouty
Supervised by :
Dr. Ashraf El Jedi
SUICIDE AND ATTEMPTED
SUICIDE
What is the suicide
Definition :
Suicide is the process of
purposely ending one's own life.
The way societies view suicide varies
widely according to culture and religion. For
example, many Western cultures, as well as
mainstream Judaism, Islam, and Christianity
tend to view killing oneself as quite
negative. One myth about suicide that may
be the result of this view is considering
suicide to always be the result of a mental
illness. Some societies also treat a suicide
attempt as if it were a crime.
From most religious viewpoint suicide is
generally seen as a sin .
Other see it as a right if the condition of life
become intolerable .
The national institute for mental health
(NIMH) list of reasons that would be
suiciders give for attempting the act :
To escape from feeling of hopelessness
To escape from an intolerable situation
To change other peoples behaviour
To avoid punishment
To avoid becoming a burden
To escape from the effects of a dreaded disease
To seek martyrdom .
There are fairly distinct characteristics that
tend to discriminate between those who are
likely to complete the suicide act and those
who attempt it in order to seek help, change
other peoples attitudes or behaviour and so
on .
Completed suicides may be seen as being at
one end of the continuum with parasuicides
at the other , in the middle one can place
those persons attempting suicide with highly
lethal methods.
A number of those attempting suicide in the
middle range on the continuum do finally
complete the suicidal act at a later stage .
There are demographic and clinical
differences between the completed suicide
and parasuicides groups
Completed group:
Parasuicides group:
Older
Younger
Male
Female
Use more lethal
techniques
Suffer from a more sever
type of psychatric
disorder.
use less lethal methods
Suffer from less severe
types of psychiatric
disorders
Risk factors for the completed
suicide group
Sainsbury provides a most useful
table(12.1) summarising the main
characteristics of this group .
Klerman summary :
male more than females
Depression and affective disorders
Substance abuse
Family history of suicide
Influence of others who have completed suicide
(contagion effect).
Allebeck has reviewed the risk factors in
young men and has presented the finding
that the suicides in his group represented
indications of an antisocial personality.
Additionally interesting characteristics were:
Poor emotional control
Contact with the child welfare authorities
Contact with police
Father who used alcohol frequently
Frequent misconduct in school
Excessive use of alcohol and narcotics
Holden identifies pure depression as a
reason in young females and a hard driving
perfectionism .
Litman and Diller list three main variables
as being the chief risk factors :
(1) absent relationships of significant others {history of
social isolation and being shy}
(2) negative relationships {violent interaction}
(3) lack of resilience with normal relationships until the
experience of a sudden loss
There has been evidence in recent years of
the presence of a biochemical marker in the
form of serotonin abnormalities .
Risk factors for the attempted and
parasuicide groups
People may attempt to take their lives for
quite a number of reasons.
Often these are a cry for help , an indication
of an extreme sense of frustration.
Recent researcher {klerman & davis} have
summarised some of the main demographic
and clinical features that identify this group :
Female more than male
Recent stressful life event {ending of a relationship,
money and family problem }
Impulsivity
Feeling of being a bad person
Recent thoughts of ending life
Low lethality of method {Ex. Pills, wrist-cutting
characteristics}
Previous suicide attempts
Repetition of suicide attempt
One study (Hawton & Catalan):
Shows that 6-15% make a further attempt
within one year, with repeats being most
frequent during three months after an
attempt.
In this study :
Show that 1-2% of attempters kill themselves
in the year following and a third to a half of
those who eventually complete suicide have
a history of previous attempt.
What are the signs and
symptoms for suicide?
Warning signs that an individual is imminently
planning to kill themselves may include the
person making a will, getting his or her affairs
in order, suddenly visiting friends or family
members (one last time), buying instruments
of suicide like a gun, hose, rope or
medications, a sudden and significant decline
or improvement in mood, or writing a suicide
note.
Contrary to popular belief, many people who
complete suicide do not tell any mentalhealth professional they plan to kill
themselves in the months before they do so.
If they communicate their plan to anyone, it
is more likely to be someone with whom they
are personally close, like a friend or family
member.
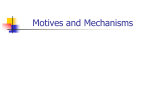
SUICIDE: A MULTI-FACTORIAL EVENT
Psychiatric Illness
Co-morbidity
Personality
Disorder/Traits
Neurobiology
Impulsiveness
Substance
Use/Abuse
Hopelessness
Severe Medical
Illness
Access To Weapons
Life Stressors
Suicide
Family History
Psychodynamics/
Psychological Vulnerability
Suicidal
Behavior
Social intervention
* It will be clear that the foregoing
demographic and clinical characteristics are
too indefinite to pinpoint precisely those who
are either going to complete suicide or to
attempt it .
* The possibilities of effective intervention in
this area must depend on such factors as
positive social policy to prevent suicide,
adequate mental health professionals to
undertake the work, public education and so
on..
The NIMH has outlined a sequence of steps
that could be the basis of successful
intervention :
{1} all suicide attempt need adequate follow up to
try to eliminate the condition that may give rise to
further attempt .
{2} close attention must be given to verbal
warnings, which may be direct or indirect .
{3} pay attention to those who are making various
changes without apparent reason, for Ex. Changing
the condition of a will.
{4} personality and behavioural changes should be
noted.
{5} identify the features of clinical depression and
take appropriate steps to deal with it.
Useful forms of social
intervention
The NIMH continues to outline a framework
for effective social intervention :
(1) listen to the person carefully .
(2) make an estimate of the extent to which the individual
has planned and prepared for the suicide event .
(3) it is vital for the listener to be really emotionally
supportive .
(4) the subject may be too confused to be able to make
sensible decisions at this time .
(5) a priority must be given to making the enviroment safe .
(6) sometimes the subject may appear to have made a quick
recovery from the trauma and even seem quite elated .
Treatment once an attempt has
taken place
Unfortunately, all too often the mental health
professional will only hear of the situation once an
attempt has been made .
Where clients are allowed to take an active role in
defining their problems.
Quite often subjects will have problems with their
spouse or de facto or with their children or other
close relatives.
It is important to test the reality of what clients are
claiming by checking things out with close
relatives and other important figures in clients
lives.
It is of vital importance to establish the extent
to which the client intended to complete the
suicidal act and the Beck Intent Scale is a
useful instrument for this purpose .
Hawton and Catalan outline a
treatment
program for the parasuicide group, focusing
upon the following factors :
•
Communication :many client lack the capacity to
discuss their needs and feeling with their partners.
• Attitude change : the clients prevailing attitudes may
be against her/his own best interests. The therapist
needs to bring out the connections between the clients
failures and these attitudes.
• Referral to special agencies for particular needs .
• Improving coping mechanisms : it is important for
the client to appreciate why he/she made this attempt.
• Provide an open access facility .
•
Prevention of suicide
•
It is doubtful whether it is feasible to take
steps to prevent suicide.
• However, a number of researchers have
proposed a range of measures, all of which
would be worthwhile and might, if fully
implemented, save lives.
• For example, the studies of the NIMH,
Allebeck and McCulloch can be used to make
suggestions for preventive intervention at a
micro and macro level.
•
Changes at the micro level
•1).
Increase the number of mental health
professionals in the community.
•2). Make better use of telephone hotline services, for
example lifeline.
•3). Educate general practitioners and other medical
personnel about the recognition of depression as a
means of reducing suicide risk.
•4). Provide increased social services at points where
suicide risks are high, for example for those clients
seen in social service departments, those clients being
interviewed by the police for offences
•
Changes at the macro level
•1). Teach
coping skills at school.
•2). Make retirement age more flexible.
•3). Provide preretirement counselling services.
•4). Ensure every elderly person has a phone and a range
of contact.
•5). Build physical barriers at places that people may use
to attempt suicide, for example tall building and bridges.
•6). Limit the number of pills on prescription.
•7). Implement tougher and more restrictive gun laws.
•8). Foster community pride and neighbourliness.
•9). Develop a better understanding of the contagion
effect in adolescent suicide.