Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Evolution of mammalian auditory ossicles wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Hearing loss wikipedia , lookup
Hearing aid wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
Outcomes for wearers of
hearing aids and improving
hearing aid technology
Harvey Dillon
NAL
CRC Hear
Denis Byrne Oration
Canberra, 2008.
Who benefits from hearing aids?
What can hearing aids do for
people with hearing loss?
How can we make hearing aids
work better?
Dillon, NAL
The bits of this talk ….
•
•
•
•
•
•
•
•
Who’s got hearing aids
Who should have hearing aids
Who’s got hearing aids but shouldn’t
How people misjudge their hearing
Why hearing aids are sometimes useless
How technology is changing candidacy
Hearing aids of the future
What we should do differently now
Dillon, NAL
Who is using hearing aids?
Of those with >25 dB 4FAHL in better ear
Use
Australia
UK
USA
23 %
Don’t have
67 %
Don’t use
10 %
Davis (2003)
Source: Blue Mountains Study (Mitchell, Hartley et al)
Kochkin (1992)
Dillon, NAL
Percentage of people with
hearing aids
Percentage penetration of hearing aids
120%
107%
100%
92%
80%
57% 55%
60%
Mitchell
(2002)
40%
20%
11%
17%
1%
0%
0-24
25-44
45-64
65-120
Hearing threshold (4FA dB HL)
Dillon, NAL
Hearing loss in the future
Sources:
Proportion of population with >=25 dB 4FAHL
ABS series B
Sth Aust population study
Percentage of
population
25.0%
20.0%
70 & over
15.0%
60-69
10.0%
50-59
5.0%
15-49
0.0%
2003
Possible further increase from:
2006
2011
2021
2031
Year
And decrease from:
Personal stereo use ↑
War exposure ↓
Rock music ↑
Manufacturing ↓
Power tools ↑
Rubella epidemics ↓
Premature baby survival ↑
Dillon, NAL
Growth in people with hearing loss
People with hearing loss (million)
(>25 dB 4FAHL better ear)
5
Blue squares =
2.5% compound
growth
4
3
2
1
0
2000
2005
2010
2015
2020
Source: Hartley & Dillon, unpublished data
2025
2030
Dillon, NAL
Growth in OHS voucher numbers
OHS vouchers issued
250,000
200,000
150,000
100,000
Blue squares = 9%
compound growth
50,000
0
2000
2002
2004
Year
2006
2008
Dillon, NAL
Penetration:
Penetratration rate
Hearing aid owners as a proportion of
those with >25 dB 4FAHL better ear
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
2000
Hearing impaired growth: 2.5%
2010
2020
2030
Year
Dillon, NAL
Conundrum
1. Older people more likely to need a
hearing aid
2. Younger people more likely to adapt well
to using a hearing aid
•
Alberti (1977); Brooks (1985)
Implication
We need to know who will benefit from a
hearing aid so those people get them as
soon as possible
Dillon, NAL
What should penetration be?
Who does benefit from a hearing
aid?
Dillon, NAL
Experiment
To determine the minimum hearing loss for which
clients will receive benefit from hearing aids.
– Previous research has not indicated a close
relationship between benefit and hearing thresholds.
– Some people with very mild losses are being fitted in
the current scheme.
– It is extremely unlikely that people with normal
hearing would benefit from hearing aids.
Should be possible to find the
minimum aidable hearing loss
Dillon, NAL
Procedure
• 400 clients sampled from OHS voucher database
– 41,521 new clients fitted Feb to Sept, 2004
• Audiometric and other details obtained from
selected clients’ files
• Questionnaire sent to selected clients
– International Outcome Inventory for Hearing Aids
– Plus 6 purpose-designed questions
• Selected clients followed up by phone or additional
mail to get a high response rate (effectively 86%)
Dillon, NAL
Percentage of population
Hearing loss characteristics of study sample
100
80
60
Better ear
Worse ear
Left fitted
Right fitted
40
20
0
0
20
40
60
80
100
120
3 FA Hearing Loss (dB)
Dillon, NAL
Usage of hearing aids
120
35%
100
80
21%
19%
60
13%
Number of clients
40
10%
20
0
None
1-4 hrs/day
>8 hrs/day
<1 hr/day
4-8 hrs/day
Q3: Daily usage
Dillon, NAL
Factor analysis of questionnaire
Factor Loadings
International
Outcomes
Inventory
for
Hearing Aids
Factor 1
Factor 2
Factor 3
Q1: want aids
0.69
0.30
0.21
Q2: difficulty unaided
0.70
0.41
0.25
Q3: use
0.74
-0.18
0.08
Q4: benefit
0.82
-0.32
0.00
Q5: residual difficulty
0.03
-0.76
-0.33
Q6: Worth it
0.83
-0.33
-0.00
Q7: Residual handicap
-0.29
-0.56
-0.06
Q8: Bother to others
-0.18
-0.68
-0.26
Q9: Quality of life
0.82
-0.32
0.02
Q10: Replace them
0.34
-0.15
-0.23
Q11: Face vision
-0.29
-0.42
0.74
Q12: paper vision
-0.22
-0.47
0.70
Proportion of variance
0.32
20
0.12
Dillon, NAL
Factor analysis of questionnaire
Factor Loadings
International
Outcomes
Inventory
for
Hearing Aids
Composite benefit
Factor 1
Factor 2
Factor 3
Q1: want aids
0.69
0.30
0.21
Q2: difficulty unaided
0.70
0.41
0.25
Q3: use
0.74
-0.18
0.08
Q4: benefit
0.82
-0.32
0.00
Q5: residual difficulty
0.03
-0.76
-0.33
Q6: Worth it
0.83
-0.33
-0.00
Q7: Residual handicap
-0.29
-0.56
-0.06
Q8: Bother to others
-0.18
-0.68
-0.26
Q9: Quality of life
0.82
-0.32
0.02
Q10: Replace them
0.34
-0.15
-0.23
Q11: Face vision
-0.29
-0.42
0.74
Q12: paper vision
-0.22
-0.47
0.70
Proportion of variance
0.32
20
0.12
Composite difficulty
Vision
Dillon, NAL
Simple correlations
People who more strongly wanted to get hearing aids:
• Use them more (Q3)
• Benefit from them more (Q4)
• Say they are worth it (Q6)
• Improve their enjoyment of life by using them (Q9)
• Would replace their hearing aids if lost (Q10)
People who had the most difficulty unaided:
• Use their hearing aids more (Q3)
• Benefit from them more (Q4)
• Say they are worth it (Q6)
• Improve their enjoyment of life by using them (Q9)
• Would replace their hearing aids if lost (Q10)
Dillon, NAL
Use
+
Benefit
+
Satisfaction
Composite
Benefit
+
QOL
Dillon, NAL
Composite benefit for different daily usage
40
11%
10%
35
9%
30
25
7%
7%
20
15
4%
4%
10
2%
Number of people
5
1%
0
0.5
1.5
1.0
0% 0% 0% 0% 0% 0%
2.5
2.0
3.5
3.0
4.5
4.0
5.5
0%
3%
2% 2%
1%
0.5
5.0
3%
0% 0% 0% 0%
1.5
1.0
2.5
2.0
No use
3.5
3.0
4.5
4.0
5.5
5.0
0% 0% 0%
0.5
1.5
1.0
<1 hour per day
0% 0%
2.5
2.0
3.5
3.0
4.5
4.0
5.5
5.0
1 to 4 hours per day
40
35
30
25
6%
20
15
5%
4%
4%
10
5
0
0% 0%
1% 0%
1.5
0.5
1.0
2% 2%
2%
1%
0%
2.5
2.0
3.5
3.0
High use goes with
high benefit and
vice-versa
6%
4.5
4.0
4 to 8 hours per day
5.5
5.0
0% 0% 0%
1% 0%
1.5
0.5
1.0
2.5
2.0
0%
3.5
3.0
4.5
4.0
>8 hours per day
5.5
5.0
Dillon, NAL
What might account for variation in
benefit?
•
•
•
•
•
•
•
Hearing loss
Age
Gender
Type of hearing aid
Difficulty listening unaided
Original desire to get hearing aids
Visual ability
Dillon, NAL
Difficulty hearing unaided and wish to get hearing aids
60
50
40
30
20
10
0
1
2
3
4
5
Q2: No dif f iculty unaided
1
2
3
4
5
Q2: Slight dif f iculty unaided
1
2
3
4
5
Q2: Moderate dif f iculty unaided
60
No of obs
50
40
30
20
10
0
1
2
3
4
5
Q2: Quite a lot of dif f iculty unaided
1
2
3
4
5
Unaided difficulty
related to wish to get
hearing aids
Q2: Very much dif iculty unaided
Q1: Want hearing aids
Dillon, NAL
Difficulty listening
unaided
+
Need
Desire to get
hearing aids
Dillon, NAL
Relationship between predictors and
outcomes
Composite
benefit
Composite
difficulty
Better ear 3FA
0.09
-0.18
Worse ear 3FA
0.13
-0.17
Better ear 4FA
0.08
-0.23
Worse ear 4FA
0.13
-0.20
Age
-0.15
0.03
Need strength
0.51
-0.44
Vision summary
-0.08
0.19
Only self-assessed need predicts outcomes
Dillon, NAL
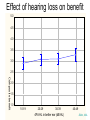
Effect of hearing loss on benefit
5.0
4.5
4.0
3.5
3.0
2.5
Composite benefit
2.0
1.5
1.0
10-19
20-29
30-39
4FA HL in better ear (dB HL)
40-49
Dillon, NAL
Effect of hearing loss on benefit
5.0
4.5
Composite benefit
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0-9.9
20-29.9
10-19.9
40-49.9
30-39.9
60-69.9
50-59.9
Poorer ear 3FA range (dB HL)
Dillon, NAL
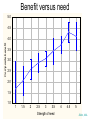
How is composite benefit related to need?
Dillon, NAL
Benefit versus need
5.0
4.5
Composite benefit
4.0
3.5
3.0
2.5
2.0
1.5
1.0
1
1.5
2
2.5
3
3.5
Strength of need
4
4.5
5
Dillon, NAL
“I don’t wear my hearing aids – never did.
I don’t know why they gave them to me.”
- Participant 1-089
Dillon, NAL
Benefit for different degrees of hearing loss
Current effect: F(14, 173)=.72691, p=.74537
5.0
4.5
Composite benefit
4.0
3.5
3.0
2.5
2.0
Worse ear 4FA: 20-29
Worse ear 4FA: 30-39
Worse ear 4FA: 40-49
1.5
1.0
1
1.5
2
2.5
3
Need strength
3.5
4
4.5
Dillon, NAL
Benefit for different hearing aid types
Current effect: F(12, 259)=1.3462, p=.19262
5.0
4.5
Composite benefit
4.0
3.5
3.0
2.5
2.0
1.5
ITE
BTE
ITC
1.0
1.5
2
2.5
3
Need strength
3.5
4
4.5
Dillon, NAL
Benefit for top-up and free-to-client
Top-up effect: F(8, 298)=1.2330, p=.27927
5.0
4.5
Composite benefit
4.0
3.5
3.0
2.5
2.0
1.5
Free-to-client
Top-up
1.0
1
1.5
2
2.5
3
Need strength
3.5
4
4.5
5
Dillon, NAL
Are outcomes affected by the provider the
client goes to?
Dillon, NAL
Benefit for different contractors
4.2
4.0
P=0.0004
3.8
Composite benefit
3.6
3.4
3.2
3.0
2.8
2.6
2.4
2.2
2.0
1.8
A
B
C
D
E
Contractor group
Contractor C clients get less benefit, on average
Dillon, NAL
Why?
Dillon, NAL
Hearing loss for different contractors
54
52
Worse ear 4FA (dB HL)
50
48
46
44
42
40
8 dB
38
36
34
32
30
A
B
C
D
E
Contractor group
Contractor C clients are less deaf
Dillon, NAL
Need strength for different contractors
3.8
3.6
3.4
Need strength
3.2
3.0
2.8
0.8 scale
points
2.6
2.4
2.2
2.0
1.8
A
B
C
D
E
Contractor group
Contractor C clients express less need for assistance
Dillon, NAL
Which: hearing loss or need?
• Allow for differences in hearing loss
difference in benefit remains (p=0.002)
• Allow for the differences in need
difference in benefit disappears (p=0.33)
Dillon, NAL
Benefit vs Needs applies to all contractors
Contractor C excluded
Current effect: F(8, 231)=7.0382, p=.00000
5.0
4.5
Contractors A, B, D and E
4.0
3.5
3.0
Contractor C alone
Current effect: F(7, 68)=8.7632, p=.00000
2.5
it" + "Q9: QOL")/4
5.0
2.0
Contractor C
4.5
1.5
4.0
1
1.5
2
2.5
3
3.5
4
3.5
4.5
5
Need strength
3.0
2.5
it" + "Q9: QOL")/4
Composite
Composite benefit: =("Q3: use" + "Q4: benefit" + "Q6:
1.0
2.0
1.5
1.0
1
1.5
2
2.5
3
Need strength
3.5
4
4.5
Dillon, NAL
Implication
Benefit is much more strongly determined by
need than by hearing loss.
“Need” = difficulty listening unaided + desire to get
hearing aids in first place
Dillon, NAL
Why don’t people with hearing loss
acquire hearing aids?
“My hearing loss is not bad enough to need
them” (Kochkin, 1993)
– beliefs about difficulties they are having
– beliefs about hearing aid likely benefits
– beliefs about emotional consequences of
wearing hearing aids
– beliefs about practical issues (expense,
complexity, manipulation)
Dillon, NAL
Health belief model
People act rationally, in their best interests, based on their beliefs
Selfimage
Cost
Effect on
others’ view
Inconven
-ience
Hearing aid
effectiveness
Ability to
manage
Difficulties
experienced:
frequency, severity
Hearing
loss
Dillon, NAL
Health belief model
People act rationally, in their best interests, based on their beliefs
Dillon, NAL
Health belief model
People act rationally, in their best interests, based on their beliefs
Dillon, NAL
Circle of negative beliefs
positive
I don’t
want hearing aids
Dominant community belief
Hearing aids don’t work
Tell everyone
Acquire hearing
aids anyway
“Prove” that hearing
aids don’t work
Dillon, NAL
Expectations and benefit
• Higher expectations greater use and benefit (Jerram &
Purdy, 2001)
• Higher expectations higher benefit (Cox & Alexander).
Outcomes
Use, benefit
Satisfaction
Expectations
Dillon, NAL
What can a hearing aid actually do?
1. Amplify soft sounds
2. Emphasise frontal sounds
Frequency (Hz)
125
250
500
1k
2k
4k
8k
Hearing threshold (dB HL)
0
20
40
60
80
35 dB 4FA HL
100
120
Dillon, NAL
Speech level and threshold (dB SPL)
1. Amplifying soft sounds
90.0
80.0
70.0
Speech at 55 dB SPL
60.0
50.0
40.0
30.0
20.0
10.0
100
1000
10000
Frequency (Hz)
Speech intelligibility index = 0.45 Percent words in sentences correct = 93%
Dillon, NAL
Intelligibility (% correct)
Amplifying speech
(quiet; no reverberation)
100
80
60
Unaided
Aided
40
20
0
40
50
60
70
80
Speech level (dB SPL)
People with mild to moderate loss can cope reasonably well in quiet.
Dillon, NAL
2. Speech in noise and reverberation
Noise and reverberation both usually have
biggest effect on low frequencies
Dillon, NAL
Speech level and threshold (dB SPL)
Amplifying soft sounds
90.0
80.0
70.0
60.0
Speech at 55 dB SPL
50.0
40.0
30.0
20.0
10.0
100
1000
10000
Frequency (Hz)
Speech intelligibility index = 0.45 Percent words in sentences correct = 93%
Dillon, NAL
Speech level and threshold (dB SPL)
Amplifying soft sounds
90.0
80.0
70.0
60.0
Speech at 55 dB SPL
50.0
40.0
30.0
20.0
10.0
100
1000
10000
Frequency (Hz)
Speech intelligibility index = 0.24 Percent words in sentences correct = 72%
Dillon, NAL
Solution
A directional microphone to lift the speech in
front, but not the noise
but …..
Dillon, NAL
Room acoustics
SPL
Total
Reverberant
Direct
Critical
distance
Distance
Dillon, NAL
Room acoustics
SPL
Total
Reverberant
Direct
Critical
distance
Distance
Dillon, NAL
Implication for beliefs about hearing?
Speech with no noise, no reverberation
I can understand!
My hearing is OK
Louder speech, noise, reverberation
I can’t understand
The noise makes it hard to understand,
(My hearing is fine)
Dillon, NAL
Implication for beliefs about hearing aids
Speech with no noise, no reverberation
Hearing aid helps, if needed
Close speech, directional microphone, noise &
reverberation
Hearing aid helps
Distant speech, directional microphone, noise &
reverberation
Hearing aid doesn’t help
Dillon, NAL
Impact of untreated hearing loss
Dillon, NAL
Impact of untreated hearing loss on health
• Proven links between hearing loss and:
– low mood / emotional state, greater depression
– reduced capability for self-sufficiency, restricted social
relationships
– reduced life expectancy
• Asserted links between hearing loss and:
– loneliness,
– anxiety,
– paranoia,
– exhaustion,
– insecurity,
– loss of group affiliation,
– loss of intimacy,
– anger
Dillon, NAL
Effects of hearing loss?
Hearing loss
Mortality
Cardio-vascular
disease
Depression
Activity
restriction
We just can’t deduce causation from these surveys of health
Dillon, NAL
Effects of hearing aids?
Mortality
Depression
Hearing loss
Isolation
Anxiety
Insecurity
etc
Dillon, NAL
Cross-sectional studies
Hearing loss
Better:
Less isolation.
More able to deal
with problems
Mood / less depression
Emotional state
Self-sufficiency
Social relationships
Hearing loss and hearing aids
Life expectancy
Dillon, NAL
Cross-sectional studies
Fatalistic people
Hearing loss
Better:
Mood / less depression
Pro-active people
Emotional state
Self-sufficiency
Social relationships
Hearing loss and hearing aids
Life expectancy
Dillon, NAL
Cross-sectional studies
Unwell people,
with hearing loss
Attend to
major sickness
Hearing loss
Attend to
hearing loss
Better:
Healthy people,
with hearing loss
Mood / less depression
Emotional state
Self-sufficiency
Social relationships
Hearing loss and hearing aids
Life expectancy
Dillon, NAL
Longitudinal studies
Better:
+
Social relationships
Cognitive functioning
Memory
Hearing loss
Learning ability
Less depression
Less paranoia
Mulrow et al (1990); Dye & Peak (1983)
Dillon, NAL
Aged-care facilities
Hearing loss
Appearance of dementia
Reduced
auditory
stimulation
Cognitive
decline
Actual
dementia ??
Improved services Improved quality of life
Dillon, NAL
Technology advances in the last decade
•
•
•
•
•
•
•
•
•
•
Integrated wireless receiver
Adaptive directional microphones
Multi-channel noise reduction
Feedback cancelling
Environment sensing
Wireless-linked hearing aids
Impulse noise rejection
Wax guards
Data logging
Integrated rechargeable batteries
Dillon, NAL
So why no increase in satisfaction?
• Increase in laboratory-measured benefit
• No increase in real-world reported satisfaction
Marketing, hype, cost
Technology advance
Expectations
increase
Gap between
performance and
expectations - ??
Satisfaction?
Performance
increases (a little)
Dillon, NAL
Some technology advances in the next few years
- from the CRC for Hearing, including NAL
• Trainable hearing aids
• Improved occlusion reduction
• Improved intelligibility in noise
• Hybrid cochlear implants and hearing aids
• Fully implanted devices (implants and hearing aids)?
Dillon, NAL
Moving on from prescriptions
The trainable hearing aid
Justin Zakis, Gitte Keidser,
Hugh Mcdermott, Liz Convery
Dillon, NAL
Trainable aid – general
structure
Acoustic
measurement
module
Learning
algorithms
User control(s)
Programmable amplifier
Dillon, NAL
Aid user adjusts settings...
Trainable Aid
Dillon, NAL
Aid user adjusts settings...
Trainable Aid
Dillon, NAL
...the hearing aid takes note
Trainable Aid
Dillon, NAL
Process repeats for other
sounds
Trainable Aid
Dillon, NAL
After training, preferred settings
are automatically applied...
Trainable Aid
Dillon, NAL
After training, preferred settings
are automatically applied...
Trainable Aid
Dillon, NAL
After training, preferred settings
are automatically applied...
Trainable Aid
Dillon, NAL
After training, preferred settings
are automatically applied...
Trainable Aid
Dillon, NAL
Trainable aid philosophy
Prescribe what can be prescribed,
automatically and in minimum clinical
time
Leave the rest to the client (and the
intelligence of the hearing aid)
Fine tuning
Dillon, NAL
Training gain, CT, CR.
30
Gain
Gain (dB)
25
20
CR
15
10
5
CT
0
30
40
50
60
70
80
90
Input level (dB SPL)
Dillon, NAL
Active occlusion reduction
Jorge Mejia, John Coelho (deceased)
Dillon, NAL
Electronic Venting
H/A
C
∑
A
Hearing
Aid
Canal
B
Cartilage
Dillon, NAL
Vent and amplification path transmission
Directional mic
Adaptive noise suppression
20
Insertion gain (dB)
15
Combined
path
10
5
0
-5
-10
Amplified
path
Vent path
-15
-20
125
250
500
1k
2k
4k
8k
Frequency (Hz)
Dillon, NAL
Occlusion reduction: Mean and Standard Deviation
Note that feedback gain was adjusted for all subjects, filter settings remain the same
(22 ears)
Dillon, NAL
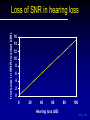
Super-directional hearing in
noise
Jorge Mejia
Dillon, NAL
Improving understanding in noise
Wireless transmission √ √ √
Directional microphones √
√
(Adaptive noise suppression)
Dillon, NAL
Physical arrangement simulated
6 mm
6 mm
Dillon, NAL
Increase in SNR needed (dB)
Loss of SNR in hearing loss
16
14
12
10
8
6
4
2
0
0
20
40
60
80
100
Hearing loss (dB)
Dillon, NAL
Blind source separation matrix
(Inverse based on initial 100 ms of signal)
Jorge Mejia
Dillon, NAL
The result ?
• Hearing impaired people who can
understand better in noise than people
with normal hearing.
Dillon, NAL
Things in your ears
• Now:
–
–
–
–
–
mobile phones,
MP3 players,
portable DVD players,
personal digital assistants,
and of course ….. hearing aids.
• In the future:
–
–
–
–
personal navigation aids,
Voice input/output internet connection,
local area (human communication) wireless networks,
……… all voice controlled, of course
Dillon, NAL
What do we mean by hearing loss?
• 2 to 3% of children are estimated to have some
form of central auditory processing disorder.
• CAPD reduces speech intelligibility in noise, just
like sensorineural hearing loss.
• CAPD includes a group of different deficits,
which can be present singly or mutiply.
• CAPD can be compensated for, and can
probably be remediated as well.
Dillon, NAL
Messages so far
• Hearing loss is on the increase due (at least) to aging
• Motivation is the major determinant of benefit
• Hearing aid penetration is:
– low, but …
– highest in world, and
– rapidly increasing.
• Fitting hearing aids to people who don’t want them
spreads negative, self-fulfilling stories
• Technology advances have been:
– worthwhile, but …
– oversold, and
– will continue, or even accelerate
Dillon, NAL
Aim
To increase penetration rate of hearing aids
and
Increase usage and benefit
Dillon, NAL
The solution is in the hands of:
•
•
•
•
•
Clinicians
Provider owners
Government
Manufacturers
Researchers
Dillon, NAL
Clinicians
Don’t fit people who don’t seem to want them
Dillon, NAL
Provider owners
Provide incentives to clinicians for superior
outcomes, not just superior sales
Dillon, NAL
Government
Pay for outcomes, not for processes
• Current system specifies process
• Payment is made for process
• Quality control inspects the process
Result:
• No control over outcomes
• No financial motivation for providers to improve outcomes
• Financial benefit if clients don’t wear hearing aids
• Financial motivation for providers to maximise number of
fittings
Dillon, NAL
Government (cont)
Alternative scheme
• Pay same for assessment
• Pay less for fitting
• Pay for outcomes
Result:
• Providers with worse than current average outcomes earn
less
• Providers with better than current average outcomes earn
more
• Most providers will have better than current average
outcmes
• Huge saving by government on people who won’t be fitted
Dillon, NAL
Government (cont)
Outcomes measurement
Just measure:
–
–
–
–
Use
Benefit
Satisfaction
Quality of life improvement
International Outcomes
Inventory for Hearing Aids
Need to allow for:
– New versus return clients
– Response rate
– Degree of hearing loss
Dillon, NAL
Manufacturers
• Continue technology improvements
• Change marketing:
– don’t oversell;
– don’t confuse
• Pursue convergence
–
–
–
–
hearing aid
communication device
hearing protector
better than normal hearing
hearing aids
normalised
and desired
Dillon, NAL
Hearing device of the future
• Pathway to many systems:
Communication
Information
Entertainment
• Speech enhancer in noise
• Active hearing protector
• (Hearing aid)
Dillon, NAL
Noise
suppression
Adaptive
directionality
Feedback
cancelling
Bernafon
Oticon
Phonak
Siemens
Starkey
Dillon, NAL
Researchers
• What makes a hearing aid candidate ?
– What other than motivation ?
– How do you measure motivation ?
– How do you change motivation ?
• How beneficial are hearing aid features ?
– For different people
– For different situations
Dillon, NAL
Future behavioural research
• Why don’t some people seek help?
• Why do some people seeking help not get
hearing aids?
• Why do some who get hearing aids not get
benefit?
Dillon, NAL
Results from Telscreen Testing (n=4058)
Golding, 2008
N=1270
N=1001
N=850
N=485
60.7%
38.7%
>25 dB
4FAHL
Worse ear
(Wilson et al)
N=230
27.7%
N=124
N=36
24.8%
22.9%
(N= 3996)
(age range 16-100 years only) Dillon, NAL
The life quality of people with hearing loss in the hands of:
•
•
•
•
•
Clinicians
Provider owners
Government
Manufacturers
Researchers
Dillon, NAL
Thanks for your attention
Slides will be on the NAL web site
www.nal.gov.au
From May 28
Dillon, NAL