Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
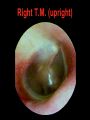
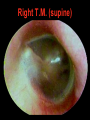
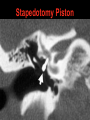
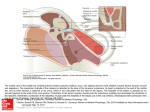
Otosclerosis Dr. Vishal Sharma Definition • Hereditary disease of bony labyrinth showing replacement of lamellar enchondral bone by irregularly laid new bone. • New bone is spongy + more vascular in active Otospongiosis but thicker & more cellular in inactive Otosclerosis. Antonio Valsalva First described ankylosis of stapes in 1741 Adam Politzer Coined the term Otosclerosis in 1893 Friedrich Siebenmann Coined the term Otospongiosis in 1912 Epidemiology • Exact etiology is unknown (? Viral) • Autosomal dominant: variable penetrance • Race: common in white races & Indians • Female : Male = 2 : 1 • Age: Common in 20 - 40 years • Hormonal influence: es in pregnancy, menopause, stress (trauma, surgery) Van der Hoeve syndrome Otosclerosis + osteogenesis imperfecta + blue sclera Types of Otosclerosis A. Stapedial B. Cochlear: otosclerotic focus is seen over Round window Promontory C. Stapedial + cochlear: mixed type D. Malignant: rapidly progressing cochlear lesion with severe sensori-neural deafness. Types of Stapedial Otosclerosis 1. Anterior focus (commonest): 2 mm anterior to oval window. 2. Posterior focus: 2 mm behind oval window. 3. Circumferential: involves footplate margin only. Types of Stapedial Otosclerosis 4. Biscuit type: footplate involved, margin is free. 5. Obliterative: obliterates oval window completely. Symptoms of Otosclerosis 1. Deafness: Bilateral, slowly progressive Conductive: stapedial otosclerosis Sensori-neural: cochlear otosclerosis Mixed: stapedial + cochlear otosclerosis 2. Soft, modulated, monotonous voice 3. Tinnitus & vertigo: in cochlear lesion Symptoms of Otosclerosis 4. Paracusis Willisii: Pt has better hearing in noisy surroundings (people increase their voice intensity & pt’s speech discrimination becomes better). Thomas Willis (1621-1675) Otoscopy Normal T.M. is seen in most cases. Pinkish colour over promontory seen in otospongiosis (2 - 10 % cases) Schwartze sign / Flamingo pink blush. Tuning Fork Tests Rinne Weber A.B.C. Stapedial Negative (BC > AC) Lateralizes to Deaf ear Normal Cochlear Positive (AC > BC) Lateralizes to Better ear Decreased Mixed Negative (BC > AC) Lateralizes to Better ear Decreased Gelle & Bing Tests Vibrating tuning fork placed over mastoid & then: External auditory canal is blocked in Bing test or E.A.C. pressure ed by Siegalization in Gelle test Bing Gelle Otosclerosis No change No change Normal / SNHL Intensity es Intensity es Pure Tone Audiometry • Low frequency conductive deafness • Carhart’s notch in bone conduction at 2 KHz Carhart’s notch • Proposed theories 1. Stapes fixation disrupts normal ossicular resonance (2000 Hz) 2. Normal compression mode of bone conduction is disturbed because of relative perilymph immobility 3. Mechanical artefact • Carhart’s notch reverses with stapes surgery Speech Audiometry Speech Discrimination Score (maximum score achieved) is almost 100 %. Speech Reception Threshold (intensity at which 50 % words are heard) is increased by the amount of conductive hearing loss. Speech Audiometry Impedance Audiometry • As curve seen in 40 % cases of otosclerosis. • Normal middle ear pressure + decreased middle ear compliance. • Others have A curve. Stapedial reflex present Stapedial reflex absent C.T. scan temporal bone 200 coronal oblique cuts are taken Stapedial otosclerosis (coronal) Cochlear otospongiosis (axial) Differential Diagnosis • Otitis Media with Effusion: type B tympanogram • Adhesive Otitis Media: absence of T.M. mobility • Tympanosclerosis: white patch on T.M. • Ossicular discontinuity: type Ad tympanogram • Congenital ossicular chain fixation: tympanotomy • Malleus head fixation: tympanotomy History of development of stapes surgery Stapes mobilization: Kessel (1880), Rosen (1952) Lateral semicircular canal fenestration: Holmgren (1923), Sourdille (1932), Lempert (1938) Complete Stapedectomy: Jack (1893), Shea (1956) Partial Stapedectomy (posterior 1/3): Plester (1960) Stapedotomy: Shea (1962), Marquet (1965) Laser Stapedotomy: Perkins & Di Bartolomeo (1980) Johannes Kessel Samuel Rosen Gunnar Holmgren Maurice Sourdille Julius Lempert John J. Shea Jr. Inclusion criteria for surgery • Pure Tone Average between 30 - 60 dB • Air bone gap > 15 dB • Speech discrimination score > 60 % • Absence of sensorineural deafness Contraindications for surgery Only hearing ear Meniere’s disease Otitis media Otitis externa Extremes of age Pregnancy Professions: divers, high construction workers, frequent travelers, noisy surroundings Surgical steps for Stapedotomy Right T.M. (upright) Right T.M. (supine) Per-meatal Incision Tympanomeatal flap raised Bony overhang curetted Bony overhang curetted Chorda tympani preserved Chorda tympani separated Confirm footplate fixation Checking for absence of round window reflex Depth measurement prosthesis Incudo-stapedial joint broken Footplate perforation made Fenestration with burr Posterior crus fractured 1 cm Teflon piston • Length of piston = medial surface of incus to stapes footplate + 0.25 mm • Range = 3.75 – 4.25 mm Piston placed in perforation Stapedius tendon cut Stapedius tendon cut Piston crimped around incus Anterior crus fractured Stapes superstructure removed Footplate perforation sealed Tympanomeatal flap put back Laser Stapedotomy Stapedius vaporization Footplate fenestration Rossette formation Stapedotomy Piston Stapedectomy Footplate Fenestration Stapes superstructure removed Footplate removal Prosthesis placed over vein graft Complications of stapes surgery Intra-operative Post-operative Floating footplate Otitis media Submerged footplate Oval window granuloma Dislocated incus Perilymph fistula Perforated TM Sensori-neural HL Damage to facial nerve Persistent air-bone gap or chorda tympani Vestibular dysfunction Persistent stapedial artery Delayed facial palsy in Perilymph flooding laser surgery Sodium Fluoride • Given in cochlear otosclerosis & active focus of otospongiosis (Schwartze sign). • Acts by: a. Decreases bone resorption b. Increases bone formation c. Prevents enzymatic damage to cochlea • 20 mg orally, thrice daily for 3 - 6 months Hearing Aid For patients who: • Are unfit for surgery • Refuse surgery Thank You