Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Outpatient commitment wikipedia , lookup
Psychological trauma wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Externalizing disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Intervention (TV series) wikipedia , lookup
Mental disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Causes of mental disorders wikipedia , lookup
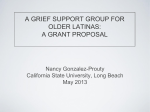
CLINICAL SOCIAL WORK IN THE 21ST CENTURY PSYCHIATRIST'S PERSPECTIVE ON AN URGENT AGENDA Dr. Katherine Shear Marion E. Kenworthy Chair Columbia University School of Social Work 24 January 2007 The Marion E. Kenworthy Lecture CLINICAL SOCIAL WORK IN THE 21ST CENTURY FROM A PSYCHIATRIST'S PERSPECTIVE Interdisciplinary Research-Practice Partnership is an Urgent Social Work Agenda CLINICAL SOCIAL WORKERS DOMINATE THE U. S. PSYCHOTHERAPY WORKFORCE 200,000 180,000 192,814 160,000 140,000 120,000 100,000 80,000 73,014 60,000 40,000 33,486 20,000 17,318 0 Clinical Social Workers Psychologists Slide provided by Myrna Weissman Ph.D. Psychiatrists Psychiatric Nurses SAMHSA 1998 OPPORTUNITIES FOR HIGH IMPACT Social workers have greater access to individuals suffering from mental disorders than any other professional group. This provides an exciting opportunity for high impact work Clinical social work is in a position to shape the mental health care system through creative utilization of research-informed assessment and intervention tools and through development of innovative models of practice-based evidence THINGS WE HAVE LEARNED Mental disorders are prevalent and debilitating Environmental factors contribute to illness and health; the most socially vulnerable are at greatest risk for developing mental disorders Both somatic and psychosocial interventions can play a role in symptom relief and building resilience However, most people do not get the help that should be available; there is an urgent need to improve care of mental disorders We need partnerships between mental health practitioners and researchers, across disciplines, to achieve this common goal THE RELATIONSHIP BETWEEN PRACTICE AND RESEARCH Clinical research can only be conducted as a partnership between research and practice. This kind of partnership needs to be expanded to include teams of dedicated clinical administrators and practitioners working with clinical and services researchers The goal is a bi-directional system with research informing practice and practice informing research THE RESEARCH-PRACTICE INTERFACE Provides •A foundation of basic science knowledge •Collection of validated clinical tools Supported by continuous infusion of research knowledge and tools RESEARCH PRACTICE Provides •Clinical observations and outcome evaluation •Generation of hypotheses Supported by ongoing communication between practitioners and researchers WHAT ARE CLINICAL TOOLS? A set of strategies and techniques targeting Alliance building to support treatment adherence Assessment, including Mental disorders and their consequences Mental health Social-environmental stresses and resources Intervention/Treatment in order to Reduce symptoms and impairments Enhance strengths Reduce environmental stress Enhance environmental resources WHAT IS IN THE RESEARCH-INFORMED CLINICAL TOOL BOX? Assessment instruments and methods to assist with a range of clinical activities, e.g. Diagnosis of clinical problems Evaluation of outcomes Decisions related to type of intervention Definitions of resilience, strengths and mental health Well-specified intervention strategies and procedures proven efficacious for target disorders and crossdisorder counseling goals Methods for employing theoretically or empirically guided strategies and techniques for use with individual clients ASSESSMENT METHODS AND INSTRUMENTS Measurement based care: a strategy for integrating assessment and treatment, entailing Implementation of regular, meaningful assessment of target symptoms or other intervention targets Use of valid reliable instrument Inclusion of assessment results in intervention decision making Most clinicians do not practice measurement-based care Many are unaware of the range of assessment instruments, their ease of administration and their potential usefulness for clinical practice EXAMPLES OF USER-FRIENDLY ASSESSMENT TOOLS PHQ-9 as a diagnostic instrument and symptom rating scale for depression Work and Social Adjustment Scale 5-item questionnaire Has been shown to be reliable and valid THE PHQ-9 Over the last 2 weeks, how often have you been bothered by any of the following problems? 1. 2. 3. 4. 5. Little interest or pleasure in doing things Feeling down, depressed, or hopeless Trouble falling asleep, staying asleep, or sleeping too much Feeling tired or having little energy Poor appetite or overeating 6. 7. 8. 9. Feeling bad about yourself, that you are a failure, or that you have let people down Trouble concentrating on things such as reading or watching television Moving or speaking very slowly or being fidgety or restless Thinking you would be better off dead or that you want to hurt yourself 2. If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? WORK AND SOCIAL ADJUSTMENT SCALE (WSAS) 1. 2. 3. 4. 5. Because of _________, my ability to work (occupational, studying, etc.) is impaired. my home management (cleaning, tidying, shopping, cooking, looking after home or children, paying bills) is impaired. my private leisure activities (done alone, such as reading, gardening, collecting, sewing, walking alone) are impaired. my social leisure activities (with other people, such as parties, bars, clubs, outings, visits, dating, home entertainment) are impaired. my ability to form and maintain close relationships with others, including those I live with, is impaired. Each item is rated on a 0-8 Scale, from “not at all” to “severe interference” Goal: Implementation of simple, user-friendly standardized assessment tools to measure outcome TREATMENT MODERATORS Moderators are client characteristics that predict outcome with one intervention compared to another Example: Attachment style as assessed with the Relationship Styles Questionnaire High attachment avoidance predicts WORSE outcome with a supportive, relationship-oriented treatment and BETTER outcome with structured CBT approach 1 Goal: Individualized treatment by employing research-informed moderators 1 McBride et.al. JCCP 2006 STRENGTHS BASED ASSESSMENT A focus on client strengths has been a mainstay of social work practice Social workers have long recognized that mental health is not simply the absence of mental disorders A growing body of research supports the importance of positive emotions, optimism and wellbeing to both mental and physical health However, systematic assessment of strengths is rarely done Many clinicians are unaware that mental health assessment instruments do exist EXAMPLE: DIAGNOSIS OF MENTAL HEALTH Criteria for a categorical diagnosis of flourishing Hedonia: high level on at least one of the following 1. Regularly cheerful, in good spirits, happy, calm and peaceful, satisfied, and full of life (positive affect past 30 days) 2. Feels happy or satisfied with life overall or domains of life (avowed happiness or avowed life satisfaction) Keyes CLM J Clin Consult Psychol 539-548 2005 MENTAL HEALTH (CONT.) Positive functioning: high level on six or more 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. of the following Positive attitudes toward oneself (self-acceptance) Positive attitude toward others (social acceptance) Insight into own potential, open to new experiences ( personal growth) Belief that people have potential and can grow (social actualization) Goals/beliefs that affirm sense of purpose and meaning ( purpose in life) Feel that one’s life is useful and valued by others (social contribution) Capability to manage complex environment, (environmental mastery) Interested in society or social life (social coherence) Guided by internal standards; resists social pressures (autonomy) Warm, satisfying relationships; empathy and intimacy (positive relations with others) Sense of belonging; comfort and support from community (social integration) Keyes CLM J Clin Consult Psychol 539-548 2005 GOAL FOR THE 21ST CENTURY: FOCUS ON PROMOTING HEALTH However measured, mental health is a concept that needs attention Mental health is not the same as the absence of mental disorder A person without a mental disorder can have a low level of mental health A person with a mental disorder can have a high level of mental health Clinicians need to evaluate both mental disorders and mental health and work simultaneously to reduce symptoms and enhance health INTERVENTION TOOLS There are now a large group of proven efficacious interventions for A range of mental disorders, e.g. Depression; Anxiety; Eating disorders; Psychotic disorders; Substance abuse, etc.) Cross-diagnosis counseling, e.g. Illness Management and Recovery; Psychoeducation; Assertive community Treatment; Supported employment Most clinicians do not utilize these tools Clinicians are often uncertain how to implement a new treatment and whether it is appropriate for their clients There is a need to find ways to employ efficacious intervention strategies as tools, used flexibly to address targeted problems USING INTERVENTION TOOLS Devising individualized treatments consisting of efficacious intervention modules, following principles of measurement-based care, may be a way to optimize intervention outcomes Our work provides an example of using the intervention “tool box” in conjunction with measurement- based care, to address a new problem WHAT WERE THESE PEOPLE EXPERIENCING? Depression? Posttraumatic stress disorder? A normal bereavement response? WE CONCLUDED THAT THIS WAS A MALADAPTIVE BEREAVEMENT RESPONSE A 4-STEP APPROACH TO CONSTRUCTING A TREATMENT Step 1: Develop a formulation of the target problem Step 2: Decide on intervention goals Step 3: Choose a set of efficacious treatment components to achieve these goals Step 4: Monitor outcome and make needed adjustments DEVELOP A FORMULATION OF THE PROBLEM Confrontation with a severely threatening reality, inconsistent with an internal working model is the hallmark of trauma We conceptualized bereavement as attachment loss that met this criterion for trauma We postulated that there are 2 generic types of trauma 1. 2. Both types of trauma entail problems comprehending the event, resulting in intrusions and avoidance 1. 2. Traumatic stress: Actual or threatened death or serious injury Traumatic loss: Permanent loss of an attachment figure Traumatic stress provokes hypervigilance to danger Traumatic loss provokes longing, searching for proximity An unresolved trauma reaction impedes the natural progress of adjustment to the severely threatening event SCHEMATIC DEPICTION OF OUR ATTACHMENTTRAUMA BASED GRIEF FORMULATION: USUAL GRIEF BEREAVEMENT (attachment loss) ACUTE GRIEF Traumatic loss reaction Caregiver selfblame Exploratory system Inhibited Transient, dominant state Painful and preoccupying Resolution of trauma (Comprehension, meaning-making, sense of controllability) Reconfiguration of the working model Positive emotions Forgiveness, compassion INTEGRATED GRIEF Permanent background state Bittersweet memories that are accessible and changing SCHEMATIC DEPICTION OF OUR FORMULATION PROLONGED (TRAUMATIC) GRIEF BEREAVEMENT (attachment loss) ACUTE GRIEF Traumatic loss reaction Caregiver selfblame Maladaptive beliefs and behaviors •Unresolved trauma •Continued yearning and searching •Dominant negative emotions Exploratory system inhibited PROLONGED (TRAUMATIC) GRIEF INTEGRATED GRIEF DECIDE ON INTERVENTION TARGETS Target Problem Negative interpretations of grief 2. Unresolved trauma 3. Maladaptive beliefs related to caregiver self-blame or survivor guilt 4. Compulsive proximity seeking 1. 2. 3. 5. Avoidance of reminders of the death 5. 1. 4. Treatment Goal Acceptance of grief Comprehension of the death Forgiveness of self and others; freedom to experience positive emotions Sense of a comfortable relationship to the deceased Reduce avoidance; Find other ways to manage emotional pain CHOOSE A SET OF INTERVENTION COMPONENTS Target Goal 1. Acceptance of grief 2. Comprehension fo the death 3. Forgiveness of self and others; freedom to experience positive emotions 4. Sense of a comfortable relationship to the deceased 5. Reduce avoidance; Find other ways to manage emotional pain 1. 2. 3. 4. 5. Treatment Component IPT: define the problem and give permission for a “sick role” CBT: Imaginal revisiting of the death; situational revisiting MET: Personal goals, self care; IPT: strengths-focused encouragement of interaction with others CBT: imaginary conversation with the deceased; memories and pictures CBT: Revisiting situations related to loss; TREATMENT PROCESS GUIDED BY BEREAVEMENT COPING THEORY Dual process theory of coping This model guided the process of the treatment Bereavement entails both loss-related and restoration-related stressors Effective coping is achieved by a process of oscillating between addressing loss and restoration All sessions focused on both loss and restoration Goal was to help the person feel comfortable with engaging the loss and also with setting it aside We added a focus on restoration-based strengths Stroebe and Schut Death Studies 23: 197–224, 1999 p.213 SUMMARY: CLINICAL PRACTICE IN THE 21ST CENTURY Research informed practice, in combination with practiceinformed research, holds great promise for enhancing the lives of people with mental disorders Goal: Utilize assessment research findings to Implement measurement-based care Inform treatment decisions using moderator variables Systematize the assessment of mental health and strengthbased care Goal: Utilize intervention research findings to individualize treatment using target symptoms or impairments defined by formulating clinical problems and defining treatment goals CONCLUSIONS This is an exciting time for clinical social workers who are in a position to lead the field in Renewed emphasis and rigor in strength-based assessment and intervention, Mental health is not the absence of mental disorder Mental disorder is not the absence of mental health Creative utilization of research informed assessment and intervention tools, and Establishment of innovative models for clinical practice and practice-based research