Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
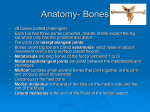
Chapter 16 Injuries to the Lower Leg, Ankle, and Foot Bones of Ankle/Lower Leg Structures of the TaloCrural (Ankle) Joint •Tibia •Medial Malleolus •Fibula •Lateral Malleolus •Talus •Interosseous Membrane Bones of Foot Foot Bones (top/superior view) Three Major Sections • Phalanges 1-5 • Proximal, distal, and intermediate • Metatarsals 1-5 • Styloid Process of 5th metatarsal • Tarsals • Calcaneus, Talus, Navicular, Cuboid, Medial Cunieform, Intermediate Cunieform, and Lateral Cunieform Medial Ligaments Ligaments of the Medial Ankle Primary ligament is: • Deltoid Ligament The deltoid ligament is the primary stabilizer of the medial side of the talocrural (ankle) joint. Lateral Ligaments Ligaments of the Lateral Ankle Primary ligaments are: • • • • Anterior talofibular (ATF) Posterior talofibular (PTF) Calcaneofibular (CF) Anterior Tibiofibular (Ant TibFib) • Posterior Tibiofibular (Post TibFib) Lateral Ligaments • These ligaments are NOT as large or strong as the deltoid. • Additional lateral stability is provided by the length of the fibula on the lateral side of the ankle. • The talocrural joint is strongest in dorsiflexion and weakest in plantar flexion (cause of many ankle sprains). Lateral Ligaments After Sprain Range of Motion (ROM) Motions of the Ankle • Dorsiflexion • Forcing foot up towards tibia • Plantarflexion • Forcing foot down away from tibia • Eversion • Forcing foot towards midline • Inversion • Forcing foot away from midline Muscles of Lower Leg/Ankle Four compartments and muscles of the lower leg/ankle • Anterior Compartment • Anterior Tibialis • Extensor Digitorum Longus • Extensor Hallicus Longus • Lateral Compartment • Peroneus Longus • Posterior Compartment • Gastrocnemius • Soleus • Plantaris • Deep Posterior Compartment • Tibialis Posterior • Flexor Digitorum Longus • Flexor Hallicus Longus Common Sports Injuries Fractures • Most often caused by direct trauma through contact. Contact causes most fractures to the lower leg and foot. • Repeated micro trauma can result in a stress fracture. • Avulsion fracture of 5th metatarsal can occur with a lateral ankle sprain. Fractures Fractures Signs and symptoms include: • Swelling and/or deformity at the site of fracture. • Discoloration at the site. • Possible broken bone end projecting through skin. • Athlete reports a snap or pop was heard or felt. • Inability to bear weight on the affected leg. For a stress fracture or growth plate fracture that did not result from traumatic event, the athlete complains of extreme point tenderness and pain at the site of injury. Fractures (cont.) First Aid • Watch and treat for shock, if necessary. • Apply sterile dressing to any open wounds. • Carefully immobilize the foot and leg using a splint. • Arrange for transport to a medical facility. Soft Tissue Injuries Ankle Injuries Ankle sprains are one of the most common injuries to this region. • Lateral sprains are more common; 80% to 85% of all ankle sprains are to the lateral ligaments (inversion sprains). • Eversion sprains, while less frequent, are often severe. Ankle Injuries: Sprains Ankle Injuries: Sprains Signs and symptoms depend on degree of sprain. • 1st degree: Pain, mild disability, point tenderness, little laxity, little or no swelling • 2nd degree: Pain, mild to moderate disability, point tenderness, loss of function, some laxity, swelling (mild to moderate) • 3rd degree: Pain and severe disability, point tenderness, loss of function, laxity, moderate to severe swelling Ankle Injuries: Sprains (cont.) First Aid • Apply ice and compression. • Elevate. • Apply a horseshoeor doughnut-shaped pad. Courtesy of Brent Mangus Ankle Injuries: Sprains (cont.) First Aid (cont.) • Have athlete use crutches with three- or four-point gait if a second- or thirddegree sprain has occurred. • If there is any question regarding the severity of the sprain, refer athlete to a medical facility for physician’s evaluation. Ankle Injuries: Sprains (cont.) Tibiofibular (tib-fib) Sprains • These injuries are often treated inappropriately as lateral ankle sprains, hindering recovery. • The difference is the mechanism of injury. Tib-fib sprains involve dorsiflexion followed by axial loading with external rotation of the foot. • Symptoms include a positive sprain test, but athlete is also in great pain. “Squeeze test” elicits pain in syndesmosis area. Ankle Injuries: Sprains (cont.) First Aid • Immediately apply ice and compression, and elevate the leg. • Apply a doughnut-shaped pad kept in place with an elastic bandage to provide compression. • Have athlete rest and use crutches for first 72 hours, followed by wearing a walking boot for 3 to 7 days. Preventing Ankle Injuries • Taping or bracing will reduce the number of ankle injuries. • Prophylactic adhesive taping supports the ankle only for a short time. • Bracing may be better than taping. • Bracing combined with some high-top shoes may be helpful. Courtesy of McDavid Tendon-Related Injuries Achilles tendon is commonly injured by longdistance runners, basketball players, and tennis players. • Onset of tendonitis may be slow among runners, but more rapid among basketball and tennis players. • Athletes who dramatically increase workout times or running distances, or who run on hard, uneven, or uphill surfaces are prone to Achilles tendonitis. The injury can be either acute or chronic. Acute injuries often associated with explosive jumping or blunt trauma. Achilles Tendonitis Achilles Tendon Injuries Signs and symptoms include: • Swelling and deformity at site of injury. • Athlete reports a pop or snap associated with the injury. • Pain in lower leg that ranges from mild to extreme. • Loss of function, mainly in plantar flexion. First Aid • Immediately apply ice and compression. • Immobilize with air cast or splint. • Arrange for transport to nearest medical facility. Compartment Syndrome Compartment syndrome usually involves the anterior compartment of the lower leg. Chronic form is related to overuse of the compartment’s muscles that causes swelling of tissues. • Acute trauma, such as being kicked in the leg, can result in swelling within the compartment as well. • In either case, swelling puts pressure on vessels and nerves. • Properly sized shin guards can protect lower leg in soccer. Compartment Syndrome (cont.) Signs and symptoms include: • Pain and swelling in the lower leg. • Athlete may complain of chronic or acute injury to the area. • There may be loss of sensation or motor control to the lower leg and/or foot. • There can be loss of pulse in the foot. • Inability to extend the big toe or dorsiflex the foot. First Aid • Apply ice and elevate. Do NOT apply compression. • If there is numbness, loss of movement, or loss of pulse to the foot, seek medical advice immediately; this is a true medical emergency. Shin Splints • “Shin splints” is a very common disorder of lower leg. Term describes exerciseinduced leg pain. • The types of activities that produce this problem and the manifestations of the injury vary depending on the athlete. • The etiology and pathology of this disorder are unclear. Shin Splints (cont.) Signs and symptoms include: • Lower leg pain either medially or posteromedially. • Typically, the athlete reports a chronic problem that progressively worsens. • Pain can be unilateral or bilateral. First Aid • Apply ice and have the athlete rest. • Use of NSAIDs may be helpful. • Athlete may need to have his or her gait analyzed for biomechanical deficiencies. • If problem worsens, athlete should seek medical advice. Plantar Fasciitis The plantar fascia is a dense collection of tissues that traverses from the plantar aspect of the metatarsal heads to the calcaneal tuberosity. • If this tissue becomes tight or inflamed by overuse or trauma, it can produce pain and disability. • Typical symptom is extreme pain in the plantar aspect of the foot with the first steps taken after getting out of bed in the morning. Pain eases with subsequent steps. • Athlete also has point tenderness in the region of the calcaneal tuberosity. Plantar Fasciitis Plantar Fasciitis (cont.) Treatment is typically conservative and includes: • Rest. • Anti-inflammatories. • Applying cold and heat alternatively to enhance healing. • A heel pad and stretching the Achilles tendon complex can assist in recovery. • Use of semirigid orthoses is also effective, but some athletes find it difficult to participate with such an orthotic in their shoes. Re-aggravating the injury increases the healing time. Heel Spurs • Heel spurs can be related to chronic plantar fasciitis. • Chronic inflammation can result in ossification at the site of attachment on the plantar aspect of the calcaneus. • Heel spurs result in long-term disability for many athletes. Treatment of Heel Spurs • Athlete should consult a physician if spurs become incapacitating. • Applying a doughnut-shaped pad beneath the heel spur may help but rarely do they ameliorate the problem. Heel Spurs Morton’s Foot Morton’s foot typically involves either a shortened 1st metatarsal or an elongated 2nd metatarsal bone. • The result shifts weight bearing to the 2nd metatarsal instead of along the 1st metatarsal. • Results in pain throughout the foot during ambulation. Morton’s Foot Morton’s Foot Morton’s foot may result in Morton’s neuroma. • The problem is usually with the nerve between the 3rd and 4th metatarsal heads. • Pain radiates to 3rd and 4th toes. • A neuroma is an abnormal growth on a nerve. • Tight-fitting shoes may be the cause. Going barefoot may help. • This condition is best cared for by a physician. Arch Problems There are two groups of arch problems: pes planus and pes cavus. • Pes planus (flat feet) related to pronation. • Excessive pronation can cause difficulties in the navicular bone and some of the joints around the ankle. • Arch taping has limited effectiveness. • Corrective arch orthoses may be beneficial. • Pes cavas (high arches) associated with plantar fasciitis and clawing of the toes. • Athlete may benefit from orthotic device. Bunions Bunions are uncommon in high school and college athletes. • Can be inflamed bursae or bone or joint deformities. • Can be caused by improperly fitting shoes. • Chronic bunion should be evaluated by physician. Bunions Blisters & Calluses Blisters and calluses are very common formations, resulting from friction between layers of skin. • When a blister forms, fluid collects between skin layers, occasionally the fluid will contain blood. • If the blister is large, it should be drained and the area padded to prevent further friction. • When draining a blister, it is best to leave top layer of skin in place. • Use sterile instruments and wear latex gloves or some other barrier to avoid contact with athlete’s body fluid. Blisters & Calluses (cont.) NSC First Aid Procedures • Wash area with soap and warm water; sterilize area with rubbing alcohol. • Use sterile needle to puncture the base of the blister and drain by applying light pressure. Process may need to be repeated during the first 24 hours. • Do not remove the top of the blister. • Apply antibiotic ointment to the top and cover with sterile dressing. • Check daily for signs of infection (redness or pus). • After 3–7 days, remove the top of blister and apply antibiotic ointment and sterile dressing. • Watch for signs of infection. Pad area with gauze pads or moleskin. Toe Injuries Common injuries are torn-off nails or hematoma formation under the nail. • Collection of blood under nail needs to be released. • Use commercially available nail bore to drill small hole in nail to release blood. Ingrown toenails may result from improperly fitting shoes. • Soak affected toe in warm antibacterial solution. • Elevate toenail by placing a small cotton roll under it and leave in place as nail grows. • Have athlete obtain shoes that fit more comfortably. Basic Taping 1. 2. 3. Basic Taping (cont.) 4. 5. 6. Basic Taping (cont.) 7. 8. 9. Basic Taping (cont.) 10. 11. 12. Basic Taping (concluded) 13. 14. 15.