Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
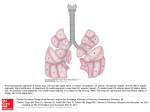
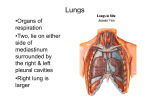
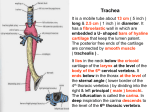
بسم هللا الرمحن الرحيم Thoracic Cavity Thoracic Cavity - The thoracic cavity consists of: I. Lung and its pleura: on each side. II. Mediastinum: In the middle part. - The mediastinum contains the heart, great vessels, and other structures. Pleura Definition: - It is a closed serous sac which is invaginated by the lung from its medial side. Layers: I. Visceral layer ----------------- Lines the surfaces and fissures of the lung. II. Parietal layer ---------------- Lines the thoracic wall and other structures. Pleura Layers: I. Visceral layer: Lines the surfaces and fissures of the lung. II. Parietal layer: Lines the thoracic wall and other structures. - Between both layers, there is a small cavity called the pleural cavity which contains minimal serous fluid. Parts of the parietal pleura: 1. Cervical pleura: protrudes through the thoracic inlet to the neck. 2. Costo-vertebral pleura: covers the inner aspect of the thoracic wall. 3. Mediastinal pleura: covers the side of the mediastinum. 4. Diaphragmatic pleura: covers the upper surface of the diaphragm. Suprapleural membrane -The cervical pleura is covered by a fibrous membrane spreading fanwise from the seventh cervical transverse process to the inner border of the first rib. Pleural recesses 1- Costo-mediastinal Recess 1 - It lies behind the sternum between the front of the thoracic wall and the mediastinum along the anterior margin of the pleura. 2- Costo-diaphragmatic 2 Recess: -It lies between the thoracic wall and the diaphragm along the lower margin of the pleura. Surface anatomy of parietal pleural (1 inch) Right pleura (1 inch) Left pleura 1-Apex of lung: It lies one inch above the medial end of the clavicle. 2-A point behind the sternal angle close to the middle line at the level of the second costal cartilage. 3-A point behind the sternum close to the middle line at the level of the fourth costal cartilage. 4- On the right side: A point behind the sternum close to the middle line at the level of the sixth costal cartilage. On the left side: A point behind the sixth costal cartilage 2 cm from the sternum. 5-A point on the eighth rib in the mid-clavicular line. 6-A point on the tenth rib in the mid-axillary line. 7-A point just below the medial end of the twelfth rib opposite the twelfth thoracic spine. Nerve supply of the pleura Parietal pleura: 1-Costal pleura and peripheral diaphragmatic pleura: Intercostal nerves . 2-Mediastinal and central diaphragmatic pleura : Phrenic nerves. Viseral pleura: Not sensitive (has autonomic nerve supply). Arterial supply Partial Pleura: 1. Intercostal arteries. 2. Internal thoracic artery. 3. Musculo-phrenic and pericardiaco-phrenic arteries. Visceral Pleura: - Bronchial arteries. Applied anatomy - Pain due to irritation of the costal and peripheral diaphragmatic pleura is referred to the thoracic or abdominal walls along the intercostal nerves. - Pain due to irritation of the mediastinal and central diaphragmatic pleura is referred to the root of the neck and shoulder, because they are supplied by the same spinal segments through the supra clavicular nerves (C. 3,4). Lung * Each lung has an apex, a base, 3 borders ( anterior, posterior and inferior), and 2 surfaces (Medial and costal). *Medial surface (Mediastinal &vertebral ) Apex And Base of the lung Apex: It extends up 1 inch above and behind the medial third of the clavicle. Base: It is concave in shape . It is related to: 1- Diaphragmatic pleura. 2- Right copula of the diaphragm. 3- Liver (right lung) . Liver, stomach (fundus), and spleen (left lung). Relations of the apex of lung Anteriorly: - Subclavian artery. Posteriorly: - The three structures which are related to the neck of the first rib (from medial to lateral): 1. Stellate ganglion. 2. Superior intercostal artery. 3. Ventral ramus of 1st thoracic n. Borders of the lung A. Anterior border It is a sharp border and occupies the costo-mediastinal recess of the pleura. The lower part of the anterior border of the left lung contains the cardiac notch (just below the cardiac notch there is a projection called the lingula). B. Posterior border It is a rounded border and occupies the para-vertebral gutter. C. Inferior border It protrudes through the costodiaphragmatic recess. Costal surface of left lung Surfaces of the lung A. Costal surface It is related to the thoracic wall and costal pleura. B.Medial surface: 1-Vertebral surface related to paravertebral gutter. 2-Mediastinal surface contains the hilum of the lung and is related to grooves and impressions. Vertebral surface . Costal surface of the lungs Right lung Left lung Lobes &Fissures of the lungs Right lung - The right lung is divided into three lobes(superior, middle, and inferior) by : 1-Oblique fissure: It begins at the posterior border of the lung opposite the fourth thoracic spine & ends at the inferior border opposite the six costo-chondral junction. 2-Transverse fissure : It begins at the anterior border opposite the fourth costal cartilage. Left lung - The left lung is divided into two lobes (superior and inferior) by the oblique fissure. * Oblique fissure (surface anatomy) - It begins at the posterior border of the lung opposite the third thoracic spine (1 inch lateral to the spine) & ends at the inferior border opposite the six costochondral junction Mediastinal Surface of the Right Lung 1- Cardiac impression, related to right atrium. 2- Superior vena cava. 3- Inferior vena cava. 4- Right innominate vein. 5- Arch of azygos vein. 6- Azygos vein. 7- Oesophagus. 8- Trachea. 9- Right vagus nerve. 10- Right phrenic nerve. 11- Ascending aorta & thymus. Mediastinal Surface of the Left Lung 1- Cardiac impression, related to left ventricle. 2- Arch of the aorta. 3- Descending aorta. 4- Left common carotid artery. 5- Left subclavian artery. 6- Oesophagus (two sites). 7- Thoracic duct. 8- Left vagus nerve. 9- Left phrenic nerve. 10- Pulmonary trunk and thymus. Hilum of the lungs * It gives passage to the structures forming the root of the lung. 1. Bronchus 2. Pulmonary artery 3. Pulmonary veins 4. Hilar lymph nodes. 5. Bronchial vessels. 6. Pulmonary plexuses (anterior and posterior). 7. Pulmonary ligament . Hilum of left lung Hilum of right lung Hilum of left lung - One bronchus( most posterior structure). -Pulmonary artery (anterior and above the bronchus -Two pulmonary veins ( most anterior and inferior structures). Hilum of right lung - Two Bronchi (Eparterial and hyparterial)( most posterior structure). - Pulmonary artery (anterior and in between the two bronchi). - Two pulmonary veins (most anterior and inferior structures). Difference between the right and left lungs 1. Size and weight Right Lung - Larger and heavier. Left Lung - Smaller and lighter. 2. Length and - Shorter and wider. breadth - Longer and narrower. 3. Lobes and fissures - Two fissures. - Three lobes. - One fissure. - Two lobes. 4. Anterior border - No cardiac notch. - Cardiac notch& lingula. 5. Hilum Broncho-pulmonary segments - The trachea divides into right and left main bronchi, with more division of the main bronchi it gives rise to lobar then segmental bronchi. - Each segmental bronchus is distributed to a localized part of lung tissue forming what is called the broncho-pulmonary segments. - The right bronchus divides into: 1- superior lobar bronchus and 2-middle and inferior lobar bronchus. Segmental branches of the bronchi Superior lobar bronchus 1. Apical 2. Anterior 3. Posterior Middle lobar bronchus Inferior lobar bronchus 4. Medial 1. Apical 2. Anterior 3. Posterior 4. Sup. lingular 5. Inf. lingular 5. Lateral 6. Apical basal 7. Medial basal 6. Apical basal 8. Lateral basal 9. Anterior basal 7. Medial basal 8. Lateral basal 10. Posterior basal 9. Anterior basal 10. Posterior basal Broncho-pulmonary segments Broncho-pulmonary segments Right lung Superior 1. Apical 2. Anterior lobe 3. Posterior Middle lobe 4. Medial Left lung 1. Apical 2. Anterior 3. Posterior 4. Sup. lingular 5. Inf. lingular 5. Lateral Inferior 6. Apical basal lobe 7. Medial basal 8. Lateral basal 9. Anterior basal 10. Posterior basal 6. Apical basal 7. Medial basal 8. Lateral basal 9. Anterior basal 10. Posterior basal Surface anatomy of the lung (and visceral pleura): -The anterior border is the same as the parietal pleura. -The inferior border: 6- A point on the six rib in the mid-clavicular line. 8- A point on the eighth rib in the mid-axillary line. 10- A point 1 inch lateral to the tenth thoracic spine. Nerve supply - Both lungs are supplied by the anterior and posterior pulmonary plexuses. a. Sympathetic component (2 - 5 thoracic sympathetic ganglia) Causes broncho-dilatation. b. Parasympathetic component (vagi) Causes bronchoconstriction + Increases the secretion of the glands. Blood supply - The lungs are supplied by the bronchial arteries ( Aorta)and drained by the bronchial veins ( Azygos system). Applied anatomy: 1. Cardiac notch of the left lung - It lies at the medial ends of the 4th and 5th intercostal spaces and related to the apex of the heart. This area is used for pericardial puncture (to aspirate fluid from the pericardium), as the introduced needle will not pass through the pleura or the lung tissue. 2. Stab wounds in the mid-axillary line a. Above the 8th rib, they lead to injury of the lung and pleura. b. Between the 10th and 8th rib, they lead to injury of the pleura. 3. Injury of the pleura leads to the followings: a. Entry of air into the pleural cavity (pneumothorax). b. Collapse of the lung tissue (atelectasis). 4. Collection of fluids in the pleura a. Serous Hydro-thorax. b. Pus Pyo-thorax. c. Blood Haemo-thorax. 5. Foreign body entering into the trachea: - It reaches the right lung because the right main bronchus is shorter, wider, and more in line with the trachea. a. If in the recumbent position: - It enters the apical segment of the inferior lobe, because it is the first posterior branch of the bronchial tree. c. If in the erect position: - It enters the posterior basal segment, because it is the most dependant branch of the bronchial tree (follows the line of gravity). Development of the respiratory system Origin: *Endoderm of foregut endothelium& glands. *Splanchnic mesoderm Ms, CT, tracheal rings. Development of the trachea Development: * Ventral border of oesophagus laryngotracheal diverticulum ( opened cranially& blind caudally) Elongates, separates from the oesophagus trachea. Bronchial tree and lung Development: *The blind caudal end of the trachea dilates gives lung bud divides into right and left buds. Development of right lung *Right lung bud three branches: 1-Upper lat. branch upper lobe bronchus . 2-Stem lower lobe bronchus. 3-Lower lat. Branchmiddle lobe bronchus. 1-Upper lobe bronchus three branches (3ry): a. Apical b. Anterior c. Posterior 2-Lower lobe bronchus five branches (3ry): a. Apical basal b. Anterior basal c.Posterior basal d. Medial basal e. Lateral basal 3- Middle lobe bronchus two branches (3ry): a.Medial b. Lateral Development of left lung *Left lung bud (1ry ) two branches: 1-One lat. Branch(2ry) upper lobe bronchus. 2-Stem lower lobe bronchus. 1-Upper lobe bronchus two branches (3ry): A-Upper: a. Apicoposterior b. Anterior B- Lower ( lingular): a. Superior b. Inferior 2-Lower lobe bronchus four branches (3ry): a. Apical basal b. Anteromedial basal c.Posterior basal d. Lateral basal • Each tertiary bronchiole divides repeatedly 18 generations. • The final generation dilates alveoli. • After birth extra 6 generations until the age of 8 years 18+ 6= 24 generations. Congenital anomalies 1- Tracheo-oesophageal fistula: No separation between the trachea and oesophagus *milk pass to the lungpneumonia. *air pass to stomach dilatation resp. impairment. 2- Variation in the number of lobes of the lung. 3- Congenital cysts of a lung: Due to dilatation of terminal bronchioles. 4- Congenital atelectasis of a lung or lobe: due to obstruction of 1ry or 2ry bronchioles. 5- Respiratory distress syndrom: Due to deficiency of surfactants secreted from type II pneumocytesno dilatation of alveoli death. Thank You Prof.: Dr. Wafaa Abdel-Rahman