Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
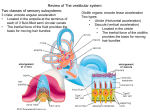
The vestibular system and cerebellum • Practical anatomy and physiology • Symptoms and signs • Clinical syndromes - diseases Flocculonodular lobe (Archicerebellum or Vestibulocerebellum) VESTIBULAR SYSTEM A central role in the maintenance of equilibrium and gaze stability. The vestibular system, by means of its receptors for the perception of linear and angular acceleration, plays a central role in orientation. Designed to answer two basic questions: Which way is up? Where am I going? VESTIBULAR SYSTEM Very elusive to test Five peripheral “receptors” (three semicircular canals, utricule, saccule) Nerve (sub-divisions) Central connections Cortical area The otoliths register linear acceleration and static tilt Vestibular system Vestibular System Vestibular Nuclei (VN) Vestibular signals originating in the two labyrinths first interact with signals from other sensory systems in the VN. Only one fraction of the neurons in the VN receive direct vestibular input, and most neurons receive afferent input from other sensory systems (visual or proprioceptive) or regions of the CNS (cerebellum, reticular formation, spinal cord and contralateral VN). Consequently the output of neurons from the VN reflect the interaction of many systems. Vestibulo-ocular and vestibulo-spinal reflexes Vestibulocerebellar and vestibulospinal pathways and connections between vestibular and ocular motor nuclei Vestibular-cerebellar connections Some fibers of the vestibular nerve transmit impulses directly via the juxtarestiform tract (next to the ICP) and runs to the flocculonodular lobe of the cerebellum. Efferents from the fastigial nucleus turn through the uncinate fasciculus of Russell back to the vestibular nuclei and via the vestibular nerve to the hair cells of the labyrinth (predominantly inhibitory) The flocculonodular lobe of the cerebellum also receives secondary fibers from the superior, medial and inferior vestibular nuclei. It returns efferent stimuli directly to the vestibular nuclei and spinal motor neurons via cerebelloreticular and reticulospinal connections. Each side of the cerebellum exerts an influence on the vestibular nuclei of both sides Vestibular Cortex Schematic representation of the temporo-peri-Sylvian vestibular cortex (TPSVC). The vestibular sites located at the lateral aspect of the right or left hemispheres are projected on a lateral view of the right hemisphere normalized in the proportional stereotactic grid system of Talairach and Tournoux. BA = Brodmann area; CA-CP = anterior commissure-posterior commissure plane; VCA = vertical plane through CA; VCP = vertical plane through CP; SF = Sylvian fissure; STS = superior temporal sulcus; 1stTG = first (superior) temporal gyrus; 2dTG = second (mid) temporal gyrus. (red dots) Yaw plane illusions; (pink dots) pitch plane illusions; (blue dots) roll plane illusions; (green dots) translations; (black dots) indefinable sensations of body motion. Vestibulo-Ocular Reflex (VOR) To hold images of the seen world steady on the retina during brief head rotations Vestibular Palsy “rapid horizontal head rotation toward the lesioned side elicits compensatory refixation saccades” CALORIC TESTING Thermal convective theory: Heating or cooling the external ear canal causes convection current in the endolymph and subsequent movement of the cupula. Vestibular Reflexes: • Vestibulospinal (VSR) – Helps maintain equilibrium - center of gravity Dizziness – Vertigo - Disequilibrium an illusion of motion implying a disorder of the vestibular system, either the peripheral labyrinth or its central connections Acute Vestibular Syndrome Severe vertigo Nausea and vomiting Nystagmus Postural instability Peripheral or central?? Hotson JR, Baloh RW, N Engl J Med 1998;339:680-5 Baloh RW, Otolaryngol Head Neck Surg 1998;119:55-9 Nystagmus due to Peripheral Acute Vestibular Syndrome • Mixed horizontal-torsional • Beats away from the side of the lesion • Increases with gaze to the quick phase • Suppressed by visual fixation • Exacerbated with affected ear down • Increased with head-shaking • Saccades and smooth pursuit preserved Peripheral Nystagmus Rt gaze Primary position Lt gaze Grade I Grade II Grade III Nystagmus due to Central Acute Vestibular Syndrome • Change direction • Not altered by visual fixation (Failure of suppression of the VOR by fixation) • Impaired saccades and smooth pursuit Central Nystagmus Rt gaze Primary position Lt gaze Types of Nystagmus Bilateral Peripheral Vestibulopathy Positive bilateral head thrust test “Negative” Romberg test “Vestibular ataxia” Ototoxicity, idiopathic, presbistasis, autoimmune disease of the inner ear Treatment: Vestibular rehabilitation Benign Paroxysmal Positional Vertigo (BPPV) Vertigo of sudden onset provoked by certain changes in head position Definite diagnosis with “positive” DixHallpike test: – A mixed torsional and vertical nystagmus – Short latency – Short duration – Fatigability Posterior canal BPPV Semont’s Liberatory Maneuver (Manoeuvre Liberatoire - 1988) Epley’s maneuver - 1992 based on canalolithiasis easy to perform short duration (5-7 min) Additional measures: vibration vestibular suppressant head in upright position for 48 hs Not necessary!!! Divisions of the Cerebellum Ventral View Superior Surface Ant Lobe flocculus nodulus Ant Lobe Post Lobe Post Lobe Midsagital View Schematic Ant Lobe nodulus Ant Lobe Post Lobe Post Lobe flocculus nodulus Cerebellar examination The main role of the cerebellum is to coordinate voluntary muscular contractions. The cerebellum adjusts the rate, regularity, and force of willed movements and regulates muscle tone. Coordination of movement is not an isolated function and is obviously influenced by the whole functioning of the nervous system. The cerebellum receives many sensory afferents as well the “brain command” of what to move. Cerebellar examination From this information the cerebellum coordinates the range, velocity and strength of contractions to produce steady volitional movements and steady volitional postures. Incoordination (ataxia) is the main feature of cerebellar dysfunction. An easy way to remember a cerebellar syndrome is to imagine a drunken person who cannot coordinate any volitional movement. He sways when standing, reels when walking, slurs words when talking and has jerky eye movements when looking. In addition, the muscles are loose and floppy (hypotonia). Cerebellar examination The incoordination of limb and trunk movements is called ataxia (from “taxis”= ordering or arranging). The incoordinated speech is called dysatrhia. The oscillations eye movements are called nystagmus. The floppiness of the extremities is called hypotonia. Thus, ataxia, dysarthria, nystagmus and hypotonia are the four major clinical signs of the cerebellar syndrome. It will be recognize that the abnormalities of speech and eye movement are of much the same nature of those of volitional movements of the limbs. Cerebellar examination Clinical examination for arm ataxia 1. Finger-to-nose test: Inspect for intention or ataxic tremor and for the accuracy to reach the nose. The cerebellar patient frequently undershoots or overshoots the target because of incoordination of agonistantagonist muscles. Such an error is called dysmetria. 2. The rapid alternating movements tests (for dysdiadochokinesia) Cerebellar examination Clinical examination for leg ataxia The heel to shin test The heel-tapping test Clinical examination for hypotonia Pendulous or hypotonic muscle stretch reflexes “Titubation”: a rhythmic “nodding” tremor of the head Clinical examination for postural or position “overshooting” The arm-pulling test Cerebellar examination Clinical examination for “cerebellar” eye movements’ abnormalities Incoordination of different eye movements that include: jerky or saccadic rather than smooth pursuit, slowness in initiating eye movements and ocular dysmetria Different types of nystagmus reflecting vestibulocerebellum dysfunction: “Gaze evoked nystagmus” (change direction in accordance to gaze direction). Other type of cerebellar nystagmus is the “rebound nystagmus” Downbeat nystagmus, opsoclonus and ocular flutter are also eye abnormalities seen in cerebellar disorders Cerebellar examination Clinical examination for cerebellar dysarthria Cerebellar speech is slurred and scanning (words are broken up into syllables), occasionally delivered with sudden unexpected force (explosive speech).