Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
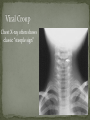
Babak Saedi MD OTOLARYNGOLOGIST TEHRAN UNIVERSITY OF MEDICAL SCIENSES Voice change Dyspnea Local pain Cough Stridor Hoarseness Retraction (intercostal- suprasternal-supraclavicular) Drooling - bleeding - emphysema History Physical examination Fiber optic laryngoscopy Radiography Arterial blood gas C.T.Scan (if general status of patient is stable) Simplest adequate form of control should be selected Lower level Other medical problems Trauma Inflammatory diseases Benign neoplasms (intrinsic – extrinsic) Malignant neoplasms (intrinsic – extrinsic) others External laryngeal injury - blunt neck trauma - penetrating wound Internal laryngeal injury - prolonged endotracheal intubation - post tracheotomy - post surgical procedures - post irradiation - endotracheal burn (thermal – chemical) CROUP AND EPIGLOTTITIS Barking Cough Hoarse Voice Inspiratory Stridor Varying Degrees of Respiratory Distress Ages infancy [1-3] (peak 2 years) Para influenza viruses – most frequent Influenza A and B – most severe (esp. A) Adenovirus Measles Respiratory syncytial virus Clinical Course: Recent URI several days before Mild cough, progressing to stridor, worsening cough, retractions. Fever usually only slightly elevated Symptoms worse at night, better in day Most gradually recover over several days Chest X-ray often shows classic “steeple sign” Management: Close observation until stable Warm or cool mist Steroids – oral or nebulized Racemic epinephrine Hospitalize hypoxic, worsening children A dramatic, potentially life-threatening form of upper airway obstruction characterized by: High fever Sore throat Dyspnea Rapidly progressive respiratory obstruction Etiology: Haemophilus influenza organism Clinical Course: Quick onset of fever, dyspnea Often sits leaning forward, drooling Inspiratory stridor Refuses to eat Within hours may progress to respiratory obstruction Can occur at any age Physical Findings: Left picture: nearly completely blocked airway Right picture: airway opened after intubation Lateral soft tissue neck xray: “thumbprint” sign TREATMENT: MAINTAIN THE AIRWAY!! Empiric antibiotics (Ceftriaxone, cefuroxime, ampicillin plus chloramphenicol) to cover most likely organisms (P mirabilis, H influenzae, E coli, K pneumoniae, and M catarrhalis) + or - Steroids Characteristic Age Onset Location Temperature Dysphagia Dyspnea Drooling Cough Position Epiglottitis Any age Sudden Supraglottic High fever Severe Present Present Uncommon Croup 6months-12yrs Gradual Subglottic Leaning forward, mouth open comfortable X-Ray Thumb sign Steeple sign Low-grade fever Mild or absent Present Present Characteristic cough Prolonged intubation Ventilation support Manage bronchopulmonary secretion Upper airway obstruction Obstructive sleep apnea Bilateral vocal cord paralysis Inability to intubate Major head & neck surgery or trauma Advantages lower risk of laryngotracheal injury improved comfort/mobility improve airway stabilization allows for oral nutrition improved secretion clearance Sternal notch Thyroid cartilage Cricoid cartilage - cricothyroid membrane - innominate artery - thyroid gland (isthmus) - recurrent laryngeal nerve Venous supply Superior and middle thyroid v. drain into the IJ Inferior thyroid v. drains into the brachiocephalic trunk Anatomy variant: thyroid ima artery, in 1.5% to 12%, in front of the trachea. Emergent (slash trach) Urgent (awake) Elective Optimally under general anesthesia Incision between sternal notch and cricoid Dissection in a vertical plane Thyroid isthmus (third and fourth ring) Entrance into trachea Tracheotomy tube insertion Hemorrhage False route Electrocautery fire Injury to adjacent structures Hemorrhage [most common ] Infection Subcutaneous emphysema Pneumomediastinum Pneumothorax [most common in infant ] Obstruction of tacheotomy tube Displacement of tube Hemorrhage Tracheoesophageal fistula Tracheal stenosis Tracheocutaneous fistula