Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
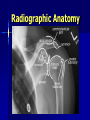
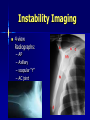
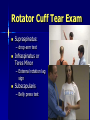
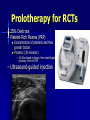
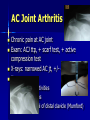
COMMON SHOULDER PROBLEMS Kevin deWeber, MD, FAAFP, FACSM Director, Sports Medicine Fellowship USUHS Objectives Review anatomy – Makes for better diagnoses Discuss common shoulder problems Describe current treatments Anatomy Scapula – – – – – – – Glenoid Acromion Coracoid Subscapular fossa Scapular spine Supraspinous fossa Infraspinous fossa Anatomy Bursae – Subacromial (Subdeltoid) – Subscapular Joints of the Shoulder Acromioclavicular Glenohumeral Sternoclavicular Scapulothoracic – Not a “true” joint Movement control Flexion: Pectoralis Major, Deltoid (Anterior), Coracobrachialis Extension: Deltoid (Posterior), Teres Major Abduction: Deltoid, Supraspinatus Adduction: Pectoralis Major, Latissimus, Subscapularis, Infrapspinatus, Teres Minor Internal Rotation: Subscapularis, Pectoralis Major, Deltoid (A), Latissimus External Rotation: Infraspinatus, Teres Minor, Deltoid Shoulder: Physical Exam Inspection Palpation Range of Motion Strength Neuro-Vascular Special Tests Range of Motion Forward flexion: 160 - 180° Extension: 40 - 60° Abduction: 180◦ Adduction: 45 ° External rotation: 80 - 90 ° Internal rotation: 60 - 90 ° Strength Testing Rotator Cuff Muscles – – – – – – – S – Supraspinatus I – Infraspinatus t - Teres minor S- Supscapularis Abduction: Supra IR: subscap ER: infra, TM Other muscles – – – – Deltoid Biceps Pecs Scapular stabilizers Anatomy Muscles – – – – – – – – – Deltoid Trapezius * Rhomboids * Levator scapulae * Rotator cuff Teres major Biceps Pectoralis muscles * Serratus anterior * * Scapular stabilizers Radiographic Anatomy Common Shoulder Problems •Instability •Impingement •Rotator cuff tears •AC joint sprains and degeneration •Adhesive capsulitis •Labral tears •Biceps tendinopathy •Clavicle fractures Glenohumeral Instability – DEFINITION: painful feeling of slippage, looseness, “going in and out” Instability Eval: “FEDS” Frequency – 1-times – 2-5 – “frequent” >5 Etiology: Traumatic vs. Atraumatic Direction (predominant) – anterior – posterior – inferior Severity: Dislocation vs. Subluxation Anterior Instability Dislocation: impact to externally rotated, abducted arm Acute findings: prominent acromion, anterior fullness Special Tests: Apprehension, Relocation Anterior Dislocation Injuries Bankart Lesion – Anterior capsule torn – Anteroinferior labrum torn – Recurrent dislocations likely Hill-Sachs Lesion – Humeral compression fracture Posterior Instability Dislocations: Electrocutions, Seizures Acute findings: internal rotation, adduction Special tests: – Posterior drawer – Load-shift Inferior Instability Usually atraumatic Special tests: – Sulcus sign Instability Imaging 4-view Radiographs: – – – – AP Axillary scapular “Y” AC joint MRI Anterior Dislocation Posterior Dislocation Anterior Dislocation Reduction Attempt ASAP Intra-articular Lidocaine HELPS! Use 2-3 techniques until successful Failure: to ER – sedation Anterior Dislocation Treatment – Referral to Ortho & PhTh Surgery for younger/athletic patients Rehabilitation for others – Immobilization Sling Impingement Definition: compression of the rotator cuff in the subacromial space Symptoms: – Pain with Overhead position or flexion/Internal Rotation – Anterior, lateral shoulder pain – Night Pain Risk Factors: – – – – – Overhead activities Micotrauma GH Instability Shape of Acromion DJD Impingement Impingement screening tests Neer: full Flexion – “Neer to the Ear” Hawkins: Internal Rotation Impingement confirmatory test Full Can Test: Resistance applied in forward flexion and abduction (SCAPULAR PLANE) Neer test: Subacromial Injection relieves pain 5cc 1% lidocaine 25-27g needle Postero-laterally Wait 10 minutes for result >50% pain reduction confirms Impingement Imaging not initially needed – 4-view shoulder series – MRI if considering surgery Failed rehab Pain with ADLs Impingement Treatment Acute Phase: – – – – Avoid Exacerbating Factors Control Pain/Inflammation Physical Therapy Corticosteroid Injection Recovery Phase: ROM, Strength, Proprioception Maintenance Phase: Longer, Intense Workouts Surgical Intervention: Failed Conservative Measures, Signifcant Disability Rotator Cuff Tears Similar presentation as Impingement Failed rehab for impingement Persistent pain/weakness after Neer injection test Imaging: x-rays, MRI Rotator Cuff Tear Exam Supraspinatus: – drop-arm test Infraspinatus or Teres Minor – External rotation lag sign Subscapularis – Belly press test Rotator Cuff Tears Treatment – Conservative: Similar to Impingement – Surgical: Young patient, large tears, dominant arm Failed Conservative Therapy High-Level Athlete Unable to perform vocational activities Success depends upon degree of tendon damage and degeneration Ultrasound of RC tear Prolotherapy for RCTs – 25% Dextrose – Platelet-Rich Plasma (PRP) Concentration of platelets and their growth factors Process: (30 minutes) – 20-60cc blood is drawn, then centrifuged to produce 3-6ml of PRP – Ultrasound-guided injection AC Joint Sprain Mechanism: Fall on shoulder Presentation: superior shoulder pain Exam: – AC jt TTP – +/- deformity or swelling – Cross-chest (“scarf”) test AC Joint Sprain Cross Chest (“scarf”) Test Active Compression (“AC) test AC Joint Sprain AC Joint Sprain AC Joint Sprain Imaging – Bilateral AP – Zanca View 10-15 degrees of cephalic tilt – Axillary View Evaluates clavicular displacement AC Joint Sprain: Treatment Grade I and II: Conservative – – – – Grade III: Controversial; refer to Ortho for counseling – – – – Immobilization Ice, Analgesics ROM, Strengthening Anesthetic injection if rapid RTP needed Immobilization for up to 4 weeks Most studies indicate conservative treatment is better Surgical management with higher rate of complications1 Conservative management with mean time of 2.1 weeks to return to work2 Grade IV-VI: Surgical 1. Taft TN, et al. Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am 1987 2. Sep;69(7):1045-51. Auwojtys EM; Nelson G. Conservative treatment of Grade III acromioclavicular dislocations. SOClin Orthop Relat Res. 1991 Jul;(268):112-9. AC Joint Arthritis Chronic pain at AC joint Exam: ACJ ttp, + scarf test, + active compression test X-rays: narrowed AC jt, +/- osteophytes Tx: – Avoid painful activities – Steroid injections – Surgical removal of distal clavicle (Mumford) Adhesive Capsulitis Painful restriction of active and passive GH ROM Risk Factors – – – – – – – Idiopathic Diabetes Mellitus Female Gender Ages 40-60 Immobilization Inflammation Stroke Adhesive Capsulitis Stage I – 1-3 months – Pain with normal ROM Stage II: “Freezing” – 3-9 months – Pain and progressive ROM restriction Stage III: “Frozen” – 9-15 months – Severe ROM restriction with decreased pain Stage IV: “Thawing” – 15-24 months – Progressive restoration of ROM Adhesive Capsulitis: Treatment Anti-Inflammatories ROM, Stretching Steroid injection into subacromial space or GH jt Surgical – Dilatation – Manipulation Labral Tears Causes: Traction Injuries, FOOSH, Overhead motion overuse, MVA Trauma Locations: – Superior Labral AnteriorPosterior (SLAP) tear – Posterior – Anterior (from dislocation) Labral Tears History: – Pain with overhead or cross-body activity – Popping, clicking, catching – 85% incidence of coexisting pathology Physical (none diagnostic): – Crank Test – Anterior Slide Test – Yegason Test SLAP Tears Type 1: Fraying Injury Type 2: Biceps tendon detached Type 3: “Buckethandle” tear Type 4: “Buckethandle” with Biceps detached Labral Tears Diagnostic: Radiograph, MR arthrogram Treatment: – Physical Therapy for > 3 months – Usually don’t heal. Aim for PAIN CONTROL – Surgery: Types I and III: Debridement Types II and IV: Debridement and Reattachment – Post-Op Rehabilitation Immobilize for 3 weeks Progress with AROM Return to full activity after 12-14 weeks Biceps Tendinopathy Rarely seen in isolation – Labral tears – Rotator cuff tears – Impingement Exam findings non-specific Biceps Tendinopathy Speed’s Test: Resistance against Shoulder Flexion Yergason’s Test: Resistance against Supination Biceps Tendinopathy Treatment: – Rehab exercise – Sports Medicine referral if fails Prolotherapy injection – Refractory: MRI, surgery Clavicle Fractures Clinical Features – Clear Painful event – Pain with arm motion – Lump and possible tenting of the skin Clavicle Fractures Diagnosis – History & physical – X-ray – AP & axillary views, AP with 45° tilt – CT for proximal & distal clavicle fractures Clavicle Fractures Surgery indications: – – – – Open fracture Neurovascular compromise Displacement > shaft width Healed clavicle lump not desirable – Floating shoulder (concurrent scapular neck fracture) Clavicle Fractures Conservative tx: – Rest – Immobilization – – – – – sling proven BETTER than fig-8 Pain control, NO NSAIDs No overhead activity for 4-6 wks F/U 2-4 wks; x-rays for healing PhTh referral for rehab Surgery if fails Questions?