Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
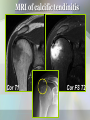
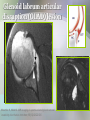
U Penn Diagnostic Imaging: On the Cape Chatham, MA – July 11-15, 2016 MRI of the Shoulder Viviane Khoury, MD Assistant Professor of Radiology University of Pennsylvania MRI of the shoulder: indications • Rotator cuff abnormalities (impingement) • Labroligamentous/ biceps pulley abnormalities (glenohumeral joint instability, internal impingement) Rotator Cuff Pathology/ Shoulder Impingement Syndrome Rotator cuff tendon pathology • Tendinopathy (tendinosis) • Partial tears • Complete tears Tendinosis • Non-inflammatory ischemic or degenerative process • Increased signal on short TE (T1, PD, GRE), less than fluid on long TE •Pitfalls: magic angle, volume averaging normal Where do cuff tears occur? • Most originate in supraspinatus – Anterior critical zone – May extend anteriorly to subscapularis – May extend posteriorly to infraspinatus, teres minor • “Rim rent” (supra or infraspinatus) • Posterior supraspinatus/ infraspinatus junction • Isolated infraspinatus • Isolated subscapularis (dislocations) Complete cuff tear • Direct signs: – Discontinuity of tendon – Defect filled with fluid – Tendon retraction • Indirect signs: – Fluid in subacromialsubdeltoid bursa; joint effusion – Fluid in subcoracoid bursa – Muscle atrophy, fatty infiltration Classification of complete tears according to size •Small: < 1cm •Large: 3-5 cm •Medium: 1-3 cm •Massive: >5 cm Tear morphology (arthroscopic classification) Crescent U-shaped L-shaped Burkhart SS, Lo IKY. Arthroscopic rotator cuff repair. J Am Acad Orthop Surg. 2006 Jun;14(6):333-46 Full-thickness supraspinatus tear with delamination Cor FS T2 Acute vs chronic full-thickness tear Muscle atrophy and fatty infiltration No atrophy Sag T1 Severe atrophy SS IS Sscap TM “Rim rent” tears • Partial tear at insertion on G.T. cor • Younger patients • ? Angulation of fibers at insertion • +/- Debridement sag Supraspinatus rim-rent tear cor sag Partial thickness tears • Fluid signal that does not span full thickness of tendon • May involve – Articular surface (most) – Bursal surface – Intrasubstance • Fiber discontinuity, fraying, change of tendon caliber Bursal surface partial thickness tear Cor Sag Grading of partial tears • Grade 1: < 3mm (<25%) • Grade 2: 3-6 mm (25-50%) • Grade 3: > 6mm (>50%) (normal cuff: 10-12 mm thick) • Grade influences surgical decision • Grading may be difficult with arthroscopy “PASTA” lesion (Partial articular surface supraspinatus tendon avulsion) 49M delamination Grade 1 partial tear MR-arthrography improves conspicuity of partial tears Low-grade articular surface partial supraspinatus tear (27M athlete) Fat sat T2 Fat sat T1 Bursal surface partial tear: (MR-arthrography pitfall) FS T1 FS T2 Rotator interval : biceps pulley • Between supraspinatus and subscapularis: – SGHL – Coracohumeral ligament – LHB • Role in glenohumeral joint stability Habermeyer P, et al. Anterosuperior impingement of the shoulder as a result of pulley lesions: A prospective arthroscopic study. J Shoulder Elbow Surg 2004 Rotator cuff interval pathology •Acute trauma •Chronic anterior instability •Diffuse degenerative process •Adhesive capsulitis Morag Y, Jacobson JA, Shields G, et al. MR arthrography of rotator interval, long head of the biceps brachii, and biceps pulley of the shoulder. Radiology 2005 Apr;235(1):21-30 N Acute rotator interval tear Sag FS T1 Morag Y, Jacobson JA, Shields G, et al. MR arthrography of rotator interval, long head of the biceps brachii, and biceps pulley of the shoulder. Radiology 2005 Apr;235(1):21-30 RI and biceps brachii instability • Biceps dislocations are accompanied by ligamentous pulley tears • Different patterns of LHB dislocations depending on lesions of CHL, SGHL, subscapularis Shoulder Impingement Syndrome: Contributing factors • • • • Acromion morphology AC joint OA Os acromiale Thick coracoacromial ligament/ subacromial enthesophyte • Post-traumatic bony deformity • Muscular hypertrophy • … MRI of calcific tendinitis Cor T1 Cor FS T2 MR of the Glenoid Labrum Capsulolabral anatomy Glenohumeral joint instability • Anterior (95%) • Posterior, superior, inferior, multidirectional (5%) Bankart lesion • Detachment of anteroinferior labrum by anterior band IGHL • Disrupted scapular periosteum • “GLOM” Woertler K, Waldt S. MR imaging in sports-related glenohumeral instability. Eur Radiol 2006 Dec:16 (12):2622-36 Perthes lesion • Non-displaced labral detachment • Stripping of scapular periosteum • Best seen with MRarthrography and ABER position Wischer TK, Bredella M A, Genant HK, et al. Perthes lesion (a variant of the Bankart lesion): M R imaging and M R arthrographic findings with surgical correlation. AJR Am J Roentgenol. 2002 Jan;178(1):233-7. ALPSA (anterior labroligamentous periosteal sleeve avulsion) • Anteroinferior labrum pulled by IGHL anterior band • Periosteum intact Chronic ALPSA Hill-Sachs • Bony Bankart • HAGL lesion (humeral avulsion of [inferior] glenohumeral ligament) Glenoid labrum articular disruption (GLAD) lesion Woertler K, Waldt S. M R imaging in sports-related glenohumeral instability. Eur Radiol 2006 Dec;16(12):2622-36 “SLAP” lesions (superior labrum anterior to posterior) • Young athletes (baseball, tennis, volleyball) • Sx: sensation of instability, click, pain • Several types (4 to 10), depending on – extent of labral tear – long head of biceps involvement – glenohumeral ligament involvement sag Normal sublabral recess SLAP lesions SLAP lesion with extension into SGHL cor ax Summary: MR-arthrography indications • Main indication is evaluation of labrum / intra-articular biceps • Limited in rotator cuff pathology to – Post-operative cuff – Inconclusive MR (e.g. partial tears in young/athlete) – Suspected rotator interval tears – Suspected posterosuperior impingement Summary: Rotator cuff To include in MRI interpretation: • Condition of tendons • Size, extent, morphology of cuff tears • Involvement of contiguous structures (RI, LHB) • Contributing factors for impingement • Muscle atrophy and fatty infiltration Summary: Instability and internal impingement • MR arthrography essential; +/- ABER To include in MR-arthrogram interpretation: • Location and extent of labral tear (use clock face or quadrants) • Abnormalities of LHB and GHLs • Presence and size of Hill-Sachs, Bankart lesions • Associated rotator cuff tears (always include a fluid-sensitive sequence)