Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neglected tropical diseases wikipedia , lookup
Infection control wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Human microbiota wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Globalization and disease wikipedia , lookup
Germ theory of disease wikipedia , lookup
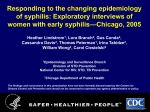
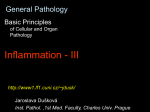
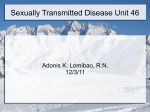
口腔微生物免疫學 Bacterial infection 細菌感染 陳玉昆教授: 高雄醫學大學 口腔病理科 07-3121101~2755 [email protected] 學習目標 Understand: 1. Virulence factor of bacteria 2. Koch postulates 3. Two main oral bacterial lesions - Caries/periapical lesions - Periodontitis 4. Tuberculosis 5. Syphilis 參考書目 References 1. Siqueira JF. Endodontic infections: Concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:281-93 2. Hoang MD et al, Secondary syphilis: a histologic and immunohistochemical evaluation. J Cutan Pathol 2004: 31: 595-9 3. Zeltser R & Kurban AK. Syphilis. Clin Dermatology 2004;22:461-8 4. Yepes JF et al, Tuberculosis: Medical management update. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:267-73 5. 結核病教學參考教材-衛生署疾病管制局 6. 黃吉志 結核病的歷史回顧與展望 高醫醫訊 94年7月 7. 張肇益 淺論牙周病病原菌、內毒素及宿主免疫反應 牙橋 2003;16:30-7 8. Slots J & Taubman MA. Contemporary oral microbiology & Immunology. First edition, 1992 Chapter 11, p. 165-190 9. Kaohsiung Medical University, Oral Pathology Department 10. Ficarra G, Carlos R. Syphilis: The renaissance of an old disease with oral implications. Head and Neck Pathol DOI 10.1007/s12105-009-0127-0 (latent/dormant) Bacterial Infection Commensal(共生) Parasite (寄生體) Pathogen(病原體) No damage Host Damage Virulence factors Adherence, extracellular enzymes, fibrinolysin, toxin Koch’s postulates The microorganism occurs in every case of the disease can account for the pathologic changes and clinical course of the disease The microorganism occurs in no other disease as a fortuitous(偶然) and nonpathogenic parasite Koch’s postulates After it is isolated from the diseased host & grown in pure culture, the microorganism can induce the disease anew Organism isolated from lesions Grown in pure culture in vitro Help! I have been infected Pure culture Animal A similar disease Organism reisolated 哈哈 Koch’s postulates Shortcomings Isolated from patients both with and without cholera(霍亂), Vibrio cholerae failed to experimentally induce the disease in animals Limitations Place considerable emphasis on pathogenicity, which resides particularly in the microorganism Dependence on host susceptibility(感受性) is an unquestionable issue Emphasize the ability to cultivate the causative microorganism in pure culture Some diseases, such as syphilis & leprosy(麻瘋), for which the causative bacterium has not yet been cultured Koch’s postulates Limitations Imply that all strains of a given microbial species are equally virulent It is known that different strains within a species vary in virulence Suggest that only a single species causes each disease There are some diseases, such as periradicular diseases, that are induced by a mixture of different microbial species Require that the suspected microorganism, after reinoculation into an animal, produce the S/S of the disease Several human pathogens either do not cause the disease in animals or cause a disease with different characteristics from the human form of the disease Two Main Bacterial Infections 牙周病 細菌 口腔兩大疾病 齲齒 病原菌: Streptococus mutans Gram (-) > 200 different microbial species can be found in infected root canals, usually in combinations of 4 to 7 species/canal Theoretically, any one of these species would have the potential to be an endodontic pathogen Requirements for endodontic pathogen (1) The microorganism must be present in sufficient number to initiate and maintain the periradicular disease The microorganism must possess an array of virulence factors, which should be expressed during root canal infection The microorganism must be spatially located in the root canal system in such a way that it or its virulence factors can gain access to the periradicular tissues The root canal environment must permit the survival and growth of the microorganism and provide signals or cues that stimulate the expression of virulence genes Requirements for endodontic pathogen (2) Inhibiting microorganisms must be absent or present in low numbers in the root canal environment The host must mount a defense strategy at the periradicular tissues, inhibiting the spread of the infection. This process will result in tissue damage Ref: 1 Two Main Bacterial Infections 牙周病 細菌 牙科 兩大 疾病 齲齒 病原菌 Specific Non- specific Specific Spirochete Amoeba 1890 1930 Bacteroides Spirochete Gram (-) A. Actinomycetemcomitans P. gingivalis P. Intermedia C. Rectus B. Forsythus 1970 1990 牙周病特定病原菌的條件 該種細菌必須能夠大量於發病時存在, 而於健康時則僅有少數或甚至沒有 該種細菌所引發之抗體價在血清,唾液 或牙齦溝液中必須要高 清除或抑制該種細菌將迅速去除或舒緩病症 病巢部的組織,若使用該種細菌之抗體來操作 螢光抗體染色法,病巢部之組織能被染色標記 該種細菌必須能夠產生致病毒素或致病原因子 該種細菌之接種必須能夠讓實驗室的無菌動物 也引發相同的病程及症狀 Principal bacteria associated with periodontal diseases Adult periodontitis Refractory periodontitis Porphyromonas gingivalis, Prevotella intermedia, B. forsythus, Campylobacter rectus Bacteroides forsythus, P. gingivalis, Campylobacter rectus, P. intermedia Localized juvenile periodontitis Periodontitis in juvenile diabetics Actinobacillus actinomycetemcomitans, Capnocytophaga Pregnancy gingivitis P. intermedia ANUG P. intermedia, Intermediate-sizedspirochetes Capnocytophaga Actinobacillus actinomycetemcomitans, 牙周病病原菌之致病力 Fimbria 牙周病病原菌 牙周組織 直接效應 Enzymes Collagense, hyaluronidase, phospholipase, phosphatases Exotoxin Endotoxin Cell inhibitors Ammonia 間接效應 Inhibition of PMN Leukotoxin, chemotaxis inhibitors, phagocytosis & intracellular killing, resistance to C-mediated killing Lymphocyte alterations Endotoxicity IgA, IgG proteases Fibrinolysin Superoxide dismutase Catalase Endotoxin - lipopolysaccharide (LPS) 化學結構 O antigen Side chain Core Polysaccharide Lipid A Core polysaccharide O antigen Lipid A polysaccharide Outer membrane Phospholipid Lipoprotein Smooth- 8-10 O antigen Semi-rough- 1-2 O antigen Peptidoglycan Inner membrane Rough- no O antigen Refs: 7,8 Endotoxin - lipopolysaccharide (LPS) 毒性強, 可直接對組織產生傷害, 亦會產生不良的免疫反應 可 : 造成 leukopenia (白細胞減少症) 活化XII blood clotting factor, 影響凝血機制 活化變異的補體反應 毒害fibroblast 引發骨吸收 活化巨噬細胞以製造IL-1,TNF-種種組織分解酶 亦產生過氧化物或離子基 Tuberulosis Aerosols Lung Granulomatous inflammation & tubercle Ghon complexe Caseation necrosis (radiodensities) (liquefy, cavitation, fibrosis & calcification) Hematogenate route Mycobacterium tuberculosis Miliary tuberculosis Koch phenomenon (partial immunity to reinfection) High lipid content Difficult to destain(退色) with acid once stained (acid-fast stain抗酸性染色) Virulence factor: Cord factor ( a glycolipid of trehalose & mycolic acid) inhibition of PMN, attack mitochondrial memb causing (no toxin) damage to respiratory &/or oxidative system, elicit granulomatous formation : PPD (purified protein derivative) Ref: 9 Caseation necrosis Ref: 5 結核桿菌(Mycobacterium tuberculosis)染色 螢光染色 抗酸性染色 Ref: 5 M tuberculosis 結核桿菌(Mycobacterium tuberculosis)結構 Bacilli Fc receptors Surfactant protein receptor High molecular Glycolipids weight lipids Mycolic acids Complement receptors CD 14 螢光染色 Aerobic Non-motile Non-spore forming Slow growing Cell Cellwall wall 抗酸性染色 Refs: 4, 9 結核病的病源 Ref: 4, 9 結核病的傳染途徑 Coughing Primary Infection Bacilli Pulmonary manifestation 80-84% Latent Active Immunosuppression Malnutrition Vitamin D deficiency Extrapulmonary manifestation 16-20% Refs: 4, 9 結核病的傳染途徑 Ref: 5 結核病的傳染途徑 只要number of cells = 10 可被感染 Ref: 5 結核病再活動的原因 Ref: 5 結 核 病 的 治 療(1) Ref: 5 結 核 病 的 治 療(2) Ref: 5 結核病 ~ 三千年歷史的古老疾病 埃及時代 西元前 3700-1000年 土偶 木乃伊(Nesperhan, priest of Amun) Ref: 5 目前全球結核病狀況 Ref: 5 2002年 各國結核病發生率比較 史瓦濟蘭 631 南非 481 菲律賓 151 越南 119 泰國 80 台灣 74.8 新加坡 36 日本 台灣肺結核 26 英國 12 瑞士 8 美國 5 冰島 3 0 10 100 1000人口 1/100,000 Bacilli Changing registration criteria New cases – 14,486 (2001) Ref: 5 臺灣結核病本國籍趨勢圖(2007-2014) 20000 病例數(人) 15000 10000 5000 0 2007 2008 2009 2010 2011 2012 2013 2014 建檔年 Ref: 5 結 核 病 防 治 原 則(1) Ref: 5 結 核 病 防 治 原 則(2) Risk Group (RG) = 3 Ref: 5 Syphilis Primary (10 days to 10 wks, average 3 wks after contact) Chancre (genitalis, oral, perineal) Lymphadenopathy (lymph node) Treponema pallidum Placenta Congenital Hutchinson triad Wassermann Ab Non-specificity IgM Index of severity Secondary (2 to 12 wks, after chancre) Generalized rash, Flu symptoms, Bone lesions (anywhere or everywhere) Tertiary (months or years after 2nd stage) Skin (gumma), CNS (tabes dorsalis), Circulatory system (aortic aneurysm) Treponemal Ab Specificity IgG Index of severity Natural history of untreated syphilis Exposure Primary incubation 10-90 days from exposure Primary syphilis Central nervous system invasion 25-60% Chancre formation Secondary incubation 4-10 weeks after chancre formation Early neurosyphilis Secondary syphilis Transmittable mother to child NonTransmittable Late latent syphilis (asymptomatic) Recurrence Transmittable sexually Early latent syphilis (asymptomatic) or mother to 1 year or less postinfection child Symptomatic in only 5% Meningitis Cranial neuritis Ocular involvement Meningiovascular disease More than 1 year postinfection Tertiary syphilis: cardiovascular syphilis Tertiary syphilis late neurosyphilis 10% (20-30 years postinfection) Tertiary syphilis: gummatous disease 15% (1-46 years postinfection) Tabes dorsalis (2-9%) (Onset 3-50 years postinfection) General paresis (2-9%) (Onset 2-30 years postinfection) Ref: 3 Natural history of untreated syphilis TERTIARY SYPHILIS Ref: 10 Constitutional and mucocutaneous manifestations of secondary syphilis Symptoms: fever, malaise, weight loss Skin rash (symmetrical and generalized), alopecia Condyloma latum in intertriginous areas Lymphadenopathy Oral involvement: multiple mucous patches covered by grayish, white pseudomembranes and surrounded by erythema Ocular involvement: uveitis, iritis, optic neuritis Arthritis, periostitis Hepatitis Glomerulonephritis Neurologic involvement: headache, meningitis, cranial nerve paralysis, cerebrovascular accident Ref: 10 Oral syphilis – re-emergence of an old disease with oral manifestations Syphilis: The Renaissance(文藝復興) of an Old Disease with Oral Implications Painless oral ulcer Oral chancer An important diagnostic criteria Ref: 3 Manifestations of untreated syphilis Chancer (頂端切平) Secondary syphilis: truncal macular- papular eruption Ref: 3 Manifestations of untreated syphilis Secondary syphilis: oral mucous patch Secondary syphilis: papular syphilis of the palms Ref: 3 Manifestations of untreated syphilis Secondary syphilis: moth-eaten alopecia(脫髮) of the scalp(頭皮) Secondary syphilis: loss of lateral eyebrow Congenital syphilis: mulberry molar Tertiary syphilis: ulcerated gumma of the leg Ref: 3 Manifestations of untreated syphilis Secondary syphilis: maculopapular skin lesions of the neck Secondary syphilis: moth-eaten alopecia Secondary syphilis: maculopapular and scaly lesions of the plantar area (浸軟) Macerated plaques (condylomata lata) of the toe webs Ref: 10 Manifestations of untreated syphilis Ulceronodular skin lesion of lue (梅毒) maligna (致命) Secondary oral syphilis: with lesions on the soft palate Secondary oral syphilis: mucous patches covered by grayish, white pseudomembranes of the lower vestibular mucosa Oral chancre in a promiscuous(淫亂) Ref: 10 woman who had unprotected oral sex Detection of spirochytes Silver stain Immunocyochemical stain Immunocyochemical stain Immunocyochemical stain Ref: 2 Summaries Knowing: 1. Virulence factor of bacteria 2. Koch postulates 3. Two main oral bacterial lesions - Caries/periapical lesions - Periodontitis 4. Tuberculosis 5. Syphilis