Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
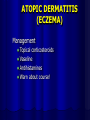
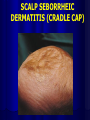
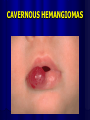
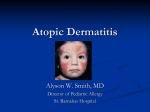
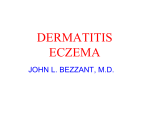
PAEDIATRIC DERMATOLOGY OBJECTIVES Common paediatric dermatologic conditions Dermatologic presentation of systemic disease Conditions which may require urgent/emergent management ASSESSMENT OF SKIN PROBLEMS History DESCRIBE WHAT YOU SEE! ASSESSMENT OF SKIN PROBLEMS History Onset, progression, change blister, bleed, drain Distribution Duration Aggravating/relieving Itch, factors pain, triggers Treatment Associated S & S e.g. fever ASSESSMENT OF SKIN PROBLEMS Past Medical History Asthma, atopy Illnesses Allergies Food, drugs, seasonal, environmental ASSESSMENT OF SKIN PROBLEMS Family History Skin disease Systemic Social Others affected at home, school or daycare Crowding, poverty 5 ITCHES 1. 2. 3. 4. 5. Dermatitis Varicella Urticaria Scabies Insect bites DERMATITIS Itching, redness, swelling, oozing, scabbing, scaling, lichenification, +blisters DERMATITIS Atopic (eczema) Diaper dermatitis Seborrheic dermatitis (cradle cap) ATOPIC DERMATITIS (ECZEMA) Site: Infant - face, scalp, extensor surfaces Child - flexor surfaces FH atopy (asthma, hayfever, anaphylaxis, allergies) Inheritance: 1 parent >60% 2 parents >80% ATOPIC DERMATITIS (ECZEMA) ATOPIC DERMATITIS (ECZEMA) Complications: Secondary bacterial infections Eczema herpeticum (herpes infecting the lesions) Prognosis: 50% clear by age 13 MANAGEMENT OF DERMATOLOGICAL PROBLEMS If it’s dry – wet it If it’s wet – dry it And if you don’t know what to do give steroids!! ATOPIC DERMATITIS (ECZEMA) Management Bathing Bath oil (e.g. Aveeno, Keri) Pat dry Ointments when wet ATOPIC DERMATITIS (ECZEMA) Management Topical corticosteroids Vaseline Antihistamines Warn about course! TOPICAL STEROIDS Weak = 1% hydrocortisone Moderate = 0.05% betamethasone 3 times a day and reduce… BEST ANTI-ITCH Hydroxyzine 0.5 mg/kg QID (max 400 mg/day) DESCRIBE WHAT YOU SEE! DIAPER DERMATITIS DIAPER DERMATITIS Contact iirritation DIAPER DERMATITIS Management Keep area dry – expose to air Protect DESCRIBE WHAT YOU SEE! CANDIDIASIS CANDIDIASIS Folds Management: Nystatin – 4 times a day/every diaper change Consider oral too Nystatin 7-10 days – 1 mL PO 4-6 times a day after food DESCRIBE WHAT YOU SEE! SCALP SEBORRHEIC DERMATITIS (CRADLE CAP) SEBORRHEIC DERMATITIS (CRADLE CAP) Occurs in any baby Sebaceous glands pump out greasy substance that keeps the old skin cells attached as it dries Greasy Yellow SEBORRHEIC DERMATITIS (CRADLE CAP) Onset most commonly in first 3 months gone by 8 to 12 months Teens often have a similar scalp condition = dandruff!! SEBORRHEIC DERMATITIS (CRADLE CAP) Management: Oil to soften/loosen scales Soft brush or dry terry cloth to brush away Consider mild topical steroid, if red/inflamed Rarer now because cleaner SCABIES Management: Permethrin 5% dermal cream – single application Neck down for 12 hours adults Include head and scalp in prepubertal Hot launder clothes from last 3 days or Seal for 48 hours Safety under 3 months not established Hydroxyzine IVERMECTIN HEAD LICE Nix (shampoo) cream rinse Nits = dead School after treatment http://www.cps.ca/ENGLISH/statements/I D/id08-06.htm BIRTH MARKS Mongolian Spots Café-au-lait spots - Transient macular stains (Salmon patches) Port wine stains MONGOLIAN SPOTS Blue/grey macula Appear at or shortly after birth Base of spine, buttocks and back Not associated with any conditions or illnesses Gradually disappear MONGOLIAN SPOTS CAFÉ-AU-LAIT SPOTS CAFÉ-AU-LAIT SPOTS Well-circumscribed, homogenously pigmented, light brown macules 1.5 - 15 cm in diameter Frequently present at birth, are almost always present by 1 year of age May increase in number during early childhood CAFÉ-AU-LAIT SPOTS Approximately 2% of all newborn infants Up to 25% of the normal adults More common in darker-pigmented races ≥6 with diameter > 0.5 cm before puberty, and 1.5 cm after puberty suggests neurofibromatosis SALMON PATCH SALMON PATCH Transient, macular Present in up to 70% of newborns Eyelids, nape of neck, glabella Most fade by 1 year of age Those in nape of neck persist in 25% of adults PORT WINE STAIN PORT-WINE STAIN Malformation of superficial capillaries of skin Pinkish/red macules Well defined edges in infancy Facial most common PORT-WINE STAIN Present at birth Permanent Variable size Do not proliferate but enlarge as child grows Lesions darken to purple and may develop a pebbly or slightly thickened surface with time MANAGEMENT Most are uncomplicated Laser therapy may help fade the lesion, best done in infancy Around eye innervated by branch 1 of trigeminal nerve – need ophthalmology assessment /neuroimaging VASCULAR MALFORMATIONS Hemangiomas Capillary (strawberry) Cavernous HEMANGIOMAS CAPILLARY (STRAWBERRY) HEMANGIOMAS Begin as flat, pale white spots & later become larger & elevated, bright red, non compressible mm - several cm Usually solitary Females 3:1 55% present at birth, rest develop later CAVERNOUS HEMANGIOMAS CAVERNOUS HEMANGIOMAS HEMANGIOMAS CAPILLARY (CAVERNOUS) Lie deeper in in skin with a slightly bluish discoloration Growth until 1 year of life Involute over 3-10 years COMPLICATIONS Peri-orbital risk to vision ( amblyopia) Ear decreased delay auditory conduction, speech Multiple cutaneous/large facial may be associated with visceral hemagiomas Subglottic hoarseness, Cosmetic stridor, respiratory failure CASE 5 week old with croup 6 day history of cough-initially harsh,loose now high pitched seal-like cough no distress, O2 sat 99%, HR 130, RR 30 erythema of left anterior tongue, left posterior palate with ? thrush …reassessment... 1 hour post epi moderate-severe respiratory distress classic “croupy” cough, RR40 severe intercostal indrawing, abd breathing, tracheal tug improved with 2nd dose epi “let’s bring her in…” admission NPO/IV/epi/steroids/ O2 unable to discontinue steroids breast feeding well limited to 10 mins no better by day 10 SIDE EFFECTS STEROIDS Cushingoid hypernatremia/hypertension/wt gain hyperglycemia adrenal suppression/immunity bone density cataracts MANAGEMENT Natural history of haemangiomata Oral systemic steroids were the mainstay of Rx if complications arise Propranolol 2 mg/kg/day INFECTIONS Fungal Bacterial TINEA CAPITIS TINEA CAPITIS Non-scarring alopecia with scales Round, scaly patches of alopecia, +/broken hairs + Boggy, elevated, discharging May be secondarily infected +/scarring TINEA CAPITIS Etiology: Fungal Investigations: Wood’s light: green fluorescence only for microsporum infections Culture of scales/hair shaft Microscopic exam of KOH preparation showing hyphae TINEA CAPITIS Management: Terbinafine (Lamisil) for 1 month 10-20 kg 62.5 mg daily 20-40 kg 125 mg daily TINEA CORPORIS (RINGWORM) TINEA CORPORIS (RINGWORM) Etiology: fungal Pruritic (not severe), scaly, round/oval plaque(s) with erythematous margin(s) and central clearing Peripheral enlargement of lesions Mostly trunk, limbs, face Contact with infected animals/pets TINEA CORPORIS (RINGWORM) Management Clotrimazole (Canesten) cream BACTERIAL INFECTIONS Impetigo Staphylococcal scalded skin syndrome (SSSS) Cellulitis Furuncle/boil IMPETIGO IMPETIGO Purulent, vesicular lesion golden yellow crust Pre-school & young adults Crowded conditions, poor hygiene, minor trauma DDx: infected eczema, HSV, varicella Organisms: Staph. Aureus, GAS, both Potential complication: poststreptococcal glomerulonephritis IMPETIGO Organisms: Staph. aureus, GAS, both Potential complication: poststreptococcal glomerulonephritis TREATMENT Topical e.g. 2% mupirocin or fucidin tid Systemic 7-10 days e.g. cephalexin 50 mg/kg divided tid/qid BULLOUS IMPETIGO Scattered, thin-walled bullae containing yellow/turbid fluid Staph. aureus Complications: Generalized skin peeling Staphylococcal Scalded Skin Syndrome STAPHYLOCOCCAL SCALDED SKIN SYNDROME (SSSS) STAPHYLOCOCCAL SCALDED SKIN SYNDROME (SSSS) CELLULITIS CELLULITIS Erythematous, flat, poorly-demarcated lesions, not uniformly raised Tender Warm Group A Strep, Staph. aureus Differential diagnosis: necrotizing fasciitis CELLULITIS TREATMENT Cephalexin q6h PO Second Cefazolin severe 50 – 100 mg/kg/d divided line = cloxacillin or clindamycin IV +/- clindamycin for FURUNCLES (BOILS) Red, hot, tender, inflammatory nodules Tense for 2-4 days, then fluctuant Yellowish point ruptures with discharge of pus Commonly around hair follicles at areas of friction & sweat nose, neck, face, axillae, buttocks MANAGEMENT Incision and Drainage Relieves pressure & pain Hot packs Antibiotic PO: e.g. cloxacillin Consider: Culture blood/pus SYSTEMIC ILLNESS Erythema multiforme Bullous erythema multiforme Toxic epidermal necrolysis (Stevens Johnson) Henoch Schonlein purpura Kawasaki disease ERYTHEMA MULTIFORME Target lesions (3 rings) HERPES SIMPLEX VIRUS Fixed (not transient e.g. giant urticaria) No pain No pruritus No scale/crust May include palms/soles May include mucosa ERYTHEMA MULTIFORME Management: Herpes isolation Oral acyclovir Topical steroids BULLOUS ERYTHEMA MULTIFORME Atypical targets Central vesicle Vesicles without targets Discrete lesions Erosions & crusts Mucous membranes involved MYCOPLASMA BULLOUS ERYTHEMA MULTIFORME Management: Admit Mycoplasma isolation Antibiotics for mycoplasma Ophthalmology, dermatology/wound oral care Systemic steroids often needed STEVENS JOHNSON SYNDROME TOXIC EPIDERMAL NECROLYSIS (STEVENS JOHNSON) Vesicles & bullae May begin as dusky papule Rapid progression Develops confluence Mucous membrane involvement Systemic involvement DRUG CAUSE USUALLY Antiepileptics Sulphurs Penicillins TOXIC EPIDERMAL NECROLYSIS (STEVENS JOHNSON) Management: Life threatening ICU/burns unit Supportive treatment History for all infections/medicines IVIG (0.75-1 g/kg/d x 3 days) Cyclosporin Steroids are controversial COURSE < 5% mortality overall Regrowth of epidermis by 3 weeks COMPLICATIONS •corneal scarring/blindness, •phimosis, vaginal synechiae (stenosis) • renal tubular necrosis •renal failure •esophageal strictures •respiratory failure •scarring/cosmetic deformity HENOCH-SCHONLEIN PURPURA “Anaphylactoid purpura” Autioimmune vasculitis Skin – petichiae, palpable, purpura Joints – arthralgia/arthritis Renal – hematuria, ↑BP, (glomerulonephritis) GI – pain secondary to edema, intussusception KAWASAKI DISEASE >80% less than age 4 Seen in all races Asian>Black>White Most common cause of acquired heart disease in children Typical vs atypical DIAGNOSTIC CRITERIA FEVER > 38.5C > 5 days PLUS 4 of: 1. EYES Bilateral non-purulent conjunctivitis 2. ‘CENTRAL’ Oral mucosal changes – fissured red lips, strawberry tongue 3. NECK Asymmetric cervical lymphadenopathy >1.5 cm 4. PERIPHERAL Desquamation (edema, erythema) 5. RASH Polymorphic Illness not explained by other (e.g. Strep/measles) ASSOCIATED FEATURES Irritability *** Arthritis Aseptic meningitis Hydrops of the gallbladder Hepatic dysfunction Diarrhea Pneumonitis Uveitis COMPLICATIONS Coronary artery ectasia/dilatation 20% if untreated 2% treated Myocarditis/pericarditis Arrhythmias TREATMENT IVIG infusion High dose then low dose aspirin Supportive SUMMARY Assessment of skin problems Itchy (2/5) Birth Marks Vascular malformations Infections Systemic illnesses REFERENCES E.O. 021.08, 021:09 and 021:11 Nelson’s Essentials of Pediatrics Color Atlas/Synopsis of Clinical Dermatology Class Handout Canadian Paediatric Society Policy Statements http://www.aboutkidshealth.ca