Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
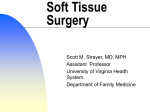
Procedures in Dermatology Overview • • • • Shave biopsy Punch biopsy Incision & Drainage (I&D) Excisions Electrodessication & Curettage (ED&C) • Cryotherapy What is a skin biopsy? • A skin biopsy is a diagnostic procedure in which a portion of skin (and/or subcutis) is submitted to the pathology lab. • This specimen is fixed, sectioned and placed on slides for histologic analysis • Special stains can be used to detect fungus, bacteria, immune complexes, lymphocytes, inflammatory mediators, arthropods. • The hope is that the pathologist can provide more information to aid in diagnosing the disease. Skin Biopsy • A good skin biopsy is one that provides an adequate specimen for the pathologist to review while at the same time using the utmost care and knowledge of anatomy to minimize the potential morbidity of the procedure. • Also involves post-biopsy wound care, knowledge of anatomical danger zones, patient education. Why do a skin biopsy? • Skin biopsies usually provide diagnostic information that adds to the clinical picture already at hand. • Many skin diseases have characteristic findings on routine histology that are highly diagnostic • Biopsy results that don’t make sense at all should be viewed with doubt – (the lab makes mistakes too!) • You might have to biopsy a lesion several times prior to definitive diagnosis. Why do a skin biopsy? • Ascertain benign vs. malignant, infectious vs. autoimmune, exogenous vs. endogenous process. • If strongly suspect skin cancer, biopsy can generate information such as subtype, differentiation, depth of invasion, type of spread, which guides appropriate choices for treatment Keep in mind, skin biopsy not necessary if…. • The clinical picture is entirely diagnostic. • If patient history and PE findings strongly point to a specific diagnosis, and you feel comfortable in diagnosing on clinical grounds alone, don’t do a skin biopsy. • If the disease doesn’t respond to treatment or doesn’t follow the expected clinical course, then biopsy may be necessary. 1- Biopsy by shave technique • Removal of representative piece of skin by tangential incision with a blade. • Can use scalpel or Dermablade • Idea is to sample both lesional and normalappearing perilesional skin • Depth needs to get down to at least superficial upper dermis – biopsies of epidermis only usually unsatisfactory. • Some skin diseases require sampling of mid to deep dermis for diagnosis. Dermablade Shave biopsy using dermablade When to do a shave • In sensitive anatomic locations where the depth of a punch biopsy puts nerves/blood vessels at risk (anatomic danger zones.) • The highly active patient: Shave biopsy wounds have no limitation on activity. • The patient who can’t/doesn’t want to come back for suture removal from punch biopsy. How to do a shave • Inform patient of potential for scarring! • Anesthetize the area for biopsy, starting with the subcutis and working you way up to the dermoepidermal junction (bleb or peau d’orange.) • Map in your mind or with a surgical pen the specimen you are trying to collect beforehand (as with many things in life/work, it helps to have a plan first!) • Create skin tension with hands or an assistant’s hands. How to do a shave • Look at Video . Shave biopsy – Wound Care • Resulting defect is usually a circular to ovular extending down into papillary to mid-reticular dermis. • Hemostasis with aluminum chloride for minimal bleeding/Electrocautery for moderate bleeding. • After hemostasis achieved, ointment and occlusive dressing are applied. • Important that patient educated on keeping would moist and occluded until healed. 2-Biopsy by punch technique • Removal of a representative piece of skin and subcutis with a punch • Best way to look at it is like a little cylindrical cookie-cutter which punches all the way through the skin • Usually a more involved procedure than shave needing extra time for anesthesia, hemostasis and would closure When to do a punch • Punch superior for any skin diseases where a picture of the deep dermis/subcutis is diagnostic. • Tends to provide more information for inflammatory skin disorders, as they tend to involve greater depth of dermis • Usually a better choice for the scar-averse patient, although it is no guarantee as even the best punch biopsy closure can dehisce. • Better choice for deeply-seated lesions in dermis and subcutis. How to do a punch • Look at video How to do a punch • Hemostasis then obtained with combination of manual pressure, electrocautery or aluminum chloride solution. • Never forget: Pressure is the King of Hemostasis! • Wound then closed with sutures, or can be left to heal by second intention (warn patient extended wound care for 1-4 weeks in these cases) 3- Excision and excional biopsy • Procedure whereby a full thickness specimen of skin is removed either for therapeutic or diagnostic purposes. • Excisions usually in elliptical shape oriented along skin tension lines (Langer’s lines.) • Suture the wound • Procedure learned by seeing/doing. • See the video Why do an excision? • Usually done to completely remove a lesion for therapeutic reasons: 1. Can also be used for excisional biopsy 2. Skin cancer 3. Dysplastic nevus (abnormal mole) 4. Epidermal inclusion cyst 4- Electrodessication and Curettage (ED&C) • Essentially a process whereby superficial cancerous and pre-cancerous growths are removed from the skin by repeated scraping and burning. • An effective, safe, expedient means of treating certain skin cancers in certain locations. Hyfrecator ED&C indications • Indicated for SCC in situ, superficial and selected nodular BCC. • Works best on trunk and extremities in nonhairbearing areas • Extreme caution on scalp, neck and highrisk areas of the face. Cryotherapy Cryotherapy: the destruction of skin lesions using a cold substance most commonly liquid nitrogen LN2 destruction is selective, affecting tissue only Cryotherapy - Indications Treatment of: Benign lesions Premalignant lesions Malignant lesions Table 1. Some of the common conditions responsive to cryosurgery. Benign lesions 8 Viral Warts 8 Skin tags 8 Seborrhoeic keratoses 8 Sebaceous hyperplasia 8 Molluscum contagiosum 8 Milia Pre-malignant lesions 8 Actinic/solar keratoses 8 Bowens disease (Intra-epithelial carcinoma) 8 Actinic cheilitis Malignant Lesions 8 Superficial basal cell carcinomas Cryotherapy - Equipment The equipment required depends on the method and technique used Methods: Open spray - 40 ̊C Cotton bud - 20 ̊C Metal forceps - 15 ̊C