Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
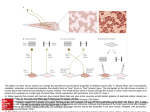
Anesthesia of patients with motor neuron disease Presentation by: SC 廖伯峰 江毅彥 History 53 y/o Female Alcohol(+), Smoking (+) 1/2 PPD General appearance: weakness Vital sign: T/P/R=36.2/84/18, BP:120/60 mmHg, Chest: Symmetric expansion. Extremities: Movable but weakness History 1.Breast tumor r/o ductal adenocarcinoma 2. Amyotrophic lateral sclerosis(2001~) 3. Gastric ulcer 4. Alcoholic with chronic pancreatitis CN I: not performed CN II: visual field – intact; visual acuity — not performed CN III, IV & VI: EOM — full CN V: facial sensation — intact CN VII: facial palsy (-) CN VIII: intact CN IX & X: gag reflex ( + /+ ) CN XI: decreased muscle power of SCM and trapezious muscle CN XII: tongue deviation (-), no atrophy or fasciculation Reflex: Babinski’s sign (-), Hoffman sign (-) Spirometry(2001) Observed Predicted %predicted FVC(L) FEV1.0(L) %FEV1.0 (%) VC(L) 2.96 2.60 87.8 2.83 2.77 2.37 85.2 2.77 106.7 109.7 RV(L) 1.68 1.73 97.4 •Normal standard spirometry • Normal diffusion capacity 102.0 Spirometry(2004) Observed Predicted %predicted FVC(L) 2.78 2.64 105.3 FEV1.0(L) 2.19 2.23 98.2 %FEV1.0 (%) 78.8 84.4 * Normal screening spirometry About motor neuron disease Selectivity of neuronal cell death—motor neuron only (except 1.ocular motility 2.parasympathetic neuron in sacral spinal cord) Light microscopy: sensory, coordination of movement, cognitive process remain intact Immunostaining: ubiquitin also in nonmotor systems—marker for degeneration Glucose metabolism About motor neuron disease Lower motor neuron (LMN): axons synapse directly on skeletal muscles Upper motor neuron (UMN): motor cortex →pyramidal tract →LMN LMN loss signs: 1) 2) 3) 4) Flaccid paralysis Fasciculations Hypotonia Hyporeflexia, areflexia UMN loss signs: 1) Initially weak and flaccid 2) Eventually spastic 3) Hypertonia 4) Hyperreflexia 5) Babinski sign Amyotrophic lateral sclerosis Amyotrophy: biopsy →muscle atrophy Lateral sclerosis: lateral column. gliosis →firmness Lou Gehrig's disease loss of anterior horn cells, the anterior (ventral) spinal motor nerve roots demonstrate atrophy epidemiology Prevelence:3 to 5 per 100,000 Western pacific Sporadic (heavy metal?) Inherited( AD): 5 to 10% Males 40 to 70 y/o (55) Median survival :3 to 5 years Amyotrophic lateral sclerosis Upper and lower motor neuron Progressive weakness Exclusion of alternative diagnosis Bulbar, cervical, thoracic, lumbosacral motor neurons 1 →possible 2 →probable 3 →definite Clinical manifestation Asymmetric weakness, usually one of distally limb first Cramping with volitional movements, typically in the morning Wasting and atrophy of muscle Fasciculation Hyperactivity of muscle stretch reflexes Difficulty of chewing, swallowing, dysarthria, exaggeration of emotion expressions Respiratory system Respiratory system Breathlessness Nocturnal hypoventilation→ morning headache, daytime hypersomnolence Poor cough Recurrent pulmonary aspiration Recurrent pneumonia Respiratory failure Die Pathogenesis Not well defined SOD1 mutation →free radical accumulations Glutamate (EAAT2, astroglial cell) VEGF↓ Discussion Anesthesia in patients with ALS Miller's anesthesia ,2005 Anesthesia and neurosurgery, 2001 Responses to muscle relaxants Bulbar dysfunction Lung function: spirometry Regional anesthesia VS general anesthesia Responses to muscle relaxants Predisposed to SCC-induced hyperkalemia because of denervation and atrophy of skeletal muscles Patient with motor neuron disease are at risk for hyperkalemia when using SCC because of upregulation of nAChRs SCC is best avoided ALS patient, in addition, presynaptic impairment of neuromuscular transmission, explains their hypersensitivity to nondepolarizing neuromuscular blockers Increased sensitivity to nondepolarizing muscle relaxants → either relaxants be avoided altogether or shorter-acting relaxants be used Bulbar dysfunction In late stage of the disease, reduced respiratory muscle reserve and abnormal airway protective reflexes → increased risk for respiratory depression and aspiration secondary to the use of sedative and anesthetic drugs Aspiration prophylaxis should be considered: no evidence Placement of a feeding tube Lung function Respiratory muscle weakness frequently develops Pre-OP ventilatory impairment may help predict anesthetic risk → one small study: 40% FVC/FEV1 Ventilatory support in the immediate post-OP period may be necessary Regional VS general anesthesia Epidural anesthesia used in ALS patients without reported untoward effect Regional anesthesia is preferable to GA RA may facilitate progression of neurodegenerative disease: evidence is anecdotal There is evidence of sympathetic hyperactivity and autonomic failure accompanied by reduced baroreflex sensitivity Handbook For Anesthesia And CoExisting Disease, 2002 Pre-OP assessment History and Examination: general details, bulbar function, respiratory function Investigations: to confirm diagnosis, routine works, chest radiography, LFT,ABG, tests of diaphragmatic function, videofluoroscopy Pre-OP management Premedication Monitoring Opioid: should be ECG avoided BP Small dose of SpO2 benzodiazepine EtCO2 Prophylaxis against Neuromuscular function pulmonary aspiration (i.e. monitoring an H2-receptor antagonist) Induction and maintenance of anesthesia Tracheal extubation should be performed with the patient fully awake to ensure maximal function of the laryngeal reflexes Regional anesthesia: if appropriate, better than GA, level of block not to compromise an already weak respiratory musculature Post-OP management Effective post-OP pain relief without the use of agents that depress respiratory Post-OP ventilation may be required and weaning may be prolonged Case report Ⅰ 46 y/o woman with emergency operation for ileus 65 y/o woman with emergency operation for gastric fistula malfunction 63 y/o man scheduled for a surgery of rectal cancer 49 y/o man scheduled for gastrectomy Spinal or/and epidural anesthesia without muscle relaxants IV propofol(3mg/kg) and sevoflurane (5%) + inhalation of 2-3% sevoflurane and single IV vecuronium 1 mg GA with sevoflurane and epidural anesthesia with lidocaine + vecuronium Case report Ⅱ Patient undergoing abdominal hysterectomy Epidural anesthesia with 2% lidocaine + continuous infusion of low dose propofol for sedation Epidural morphine provides excellent post-OP pain relief without respiratory complication Chen LK, Chang Y, Liu CC, Hou WY. Department of Anesthesiology, National Taiwan University Hospital, Taipei, R.O.C. Case report Ⅲ General anaesthesia in a patient with motor neuron disease 2004 European Academy of anaesthesiology 56 y/o man with pancreatic carcinoma scheduled for elective Whipple’s surgery 5-h operation → 8-h after, patient recovered consciousness and ventilated with CPAP → 5-h after, extubated with normal breathing pattern → 3-h after, secondary surgery → 3-h operation → 3-h after…… Without SCC: several complications Low-dose cisatracurium: may be a good choice For major surgery, using low-dose of cisatracurium and propofol is possible Repeated surgery may lead to a considerable increase in respiratory complications Spirometry should be performed and the use of neuromuscular monitoring when planning GA Case report Ⅳ Use of rapacuronium in a child with spinal muscular atrophy Paediatric anaesthesia 2001 18 month-old girl with SMA diagnosed at 6 m/o Scheduled for placement of a percutaneous jejunostomy tube Thiopental sodium, alfentanil, lidocaine for induction, and mask ventilation with 2% isoflurane Rapacuronium 9 mg (1 mg/kg) for emergency airway control Within 10 min, partial recovery of the diaphragm was observed → 20 min after, TOF responses → 75 min after, operation done Reversal with neostigmine 0.6 mg and glycopyrrolate 0.12 mg IV Guidelines are entirely based on experience with the adult form of anterior horn cell degeneration (ALS) Induction with propofol in combination with sevoflurane might have avoided laryngospasm and the use of muscle relaxants A lesser dose might have been sufficient to break laryngospasm TOF : a good monitor? Conclusion SCC is best avoided, reported to cause rhabdomyolysis and hyperkalemia from denervated muscles Use of neuromuscular monitoring when planning GA: TOF ? Muscle relaxants should be avoided altogether or shorter-acting/low-dose muscle relaxants be used