Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
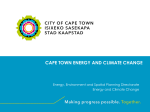
Comparison of indoor contact time data in Zambia and Western Cape, South Africa Nicky McCreesh1, Clare Looker1, Peter J. Dodd1,2, Ian D Plumb1, Kwame Shanaube3, Monde Muyoyeta3,4, Peter Godfrey-Faussett1, Elizabeth L Corbett1,5, Helen Ayles1,3, Richard G. White1 1. LSHTM, 2. University of Sheffield. 3. University of Zambia. 4. Centre for Infectious Disease Research in Zambia. 5. Malawi Liverpool Wellcome Trust Clinical Research Programme Improving health worldwide www.lshtm.ac.uk Background • We have very little idea where the majority of M.tb. transmission occurs in high incidence settings • Effective infection control measures exist, but are not widely employed outside clinics • A better understanding of important locations of transmission could inform the targeting of infection control measures, reducing M.tb. incidence • Contact data provides a starting point for identifying key locations • Aim: to compare patterns of indoor contact in urban Zambia and Western Cape, South Africa Methods • CODA study (Dodd, 2015) - cluster randomised sample of adults enrolled in ZAMSTAR final prevalence survey • Data from 3206 respondents. 40% from Western Cape, 60% from Zambia • Respondents asked about buildings entered on day before interview: • • • • Building type (shop, church, bar, etc) Duration of visit Number of adults and youth (>12 years) present Number of children (5-12 years) present • Results weighted to account for sampling design (age, gender and neighbourhood), and day of week Dodd PJ, Looker C, Plumb I, Bond G, Schaap A, Shanaube K et al. Age and gender specific social contact patterns and incidence of Mycobacterium tuberculosis infection. Am J Epidemiol. 2015;kwv160. Proportion of people who visited 30% Mean visit duration (hours) 8 25% 6 20% 15% 4 10% 2 5% 0% 0 Mean adults/youths per visit Mean children per visit 30 30 25 25 20 Adult contact hours 20 15 20 15 10 15 10 5 10 5 0 5 0 0 Western Cape Zambia p<0.05 *Estimates for bars could not be *calculated for Western Cape Proportion of people who visited 30% Mean visit duration (hours) 8 25% 6 20% 15% 4 10% 2 5% 0% 0 Mean adults/youths per visit Mean children per visit 30 30 25 25 20 Adult contact hours 20 15 20 15 10 15 10 5 10 5 0 5 0 0 Western Cape Zambia p<0.05 *Estimates for bars could not be *calculated for Western Cape Proportion of people who visited 30% Mean visit duration (hours) 8 25% 6 20% 15% 4 10% 2 5% 0% 0 Mean adults/youths per visit Mean children per visit 30 30 25 25 20 Adult contact hours 20 15 20 15 10 15 10 5 10 5 0 5 0 0 Western Cape Zambia p<0.05 *Estimates for bars could not be *calculated for Western Cape Overall adults/youths met per day Overall children met per day 4 4 3 3 2 2 1 1 0 0 Adult contact hours Child contact hours 20 20 15 10 5 Adult contact hours 15 10 20 15 5 10 0 0 5 0 Western Cape Zambia p<0.05 *Estimates for bars could not be *calculated for Western Cape Overall adults/youths met per day Overall children met per day 4 4 3 3 2 2 1 1 0 0 Adult contact hours Child contact hours 20 20 15 Adult contact hours 15 10 20 10 5 15 5 0 10 0 5 0 Western Cape Zambia p<0.05 *Estimates for bars could not be *calculated for Western Cape Discussion - limitations • Social desirability bias • No comparable data collected on public transport • Retrospective data collection, however comparable results to prospective contact diary data from Cape Town (JohnstoneRobertson, 2011; Wood 2012) Johnstone-Robertson SP, Mark D, Morrow C, Middelkoop K, Chiswell M, Aquino LD et al. Social mixing patterns within a South African township community: implications for respiratory disease transmission and control. Am J Epidemiol. 2011:kwr251 Wood R, Racow K, Bekker L-G, Morrow C, Middelkoop K, Mark D et al. Indoor social networks in a South African township: potential contribution of location to tuberculosis transmission. PLoS One. 2012;7(6):e39246. Discussion - moving from contacts to transmission risk • Contact data tell us where people spend their time and meet people • Gives some indication of locations where a substantial proportion of M.tb. is likely to occur • Doesn’t tell the whole story: • Buildings will vary in their suitability for transmission (Murray 2009, Wood 2014) • Some types of building will be visited more frequently by people who are infectious and/or highly susceptible • (Highly) infectious TB disease very rare, and large amounts of variation in susceptibility – leads to more transmission in high mixing locations Murray EJ, Marais BJ, Mans G, Beyers N, Ayles H, Godfrey-Faussett P et al. A multidisciplinary method to map potential tuberculosis transmission 'hot spots' in high-burden communities. Int J Tuberc Lung Dis. 2009;13(6):767-74 Wood R, Morrow C, Ginsberg S, Piccoli E, Kalil D, Sassi A, Walensky RP, Andrews JR (2014) Quantification of Shared Air: A Social and Environmental Determinant of Airborne Disease Transmission. PloS One 9(9): e106622. Conclusions • Patterns of indoor contact vary by setting • Targeting of infection control measures needs to be informed by local data • In Zambia, churches may be important locations for transmission. In Western Cape, indoor workplaces may be important • The potential for targeting infection control measures at these locations should be considered • More widely, a better understanding of transmission locations in different settings could improve TB control Acknowledgments • Bill and Melinda Gates Foundation • ZAMSTAR study team • LSHTM • • • • Ken Eames John Edmunds Amelia Crampin Immo Kleinschmidt • Stellenbosch University • Rory Dunbar • Study communities and participants Results Number of buildings visited 60% 50% p<0.001 40% 30% 20% 10% 0% 0 1 Western Cape 2 Zambia 3+