Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
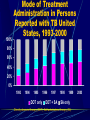
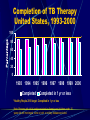
Chokechai Rongkavilit Pediatric Infectious Diseases Why do we need to know TB? Over 1/3 of world population is infected with TB. 1% of world population will become infected each year. Previous epidemic and continued immigration have resulted in a large number of latent TB in US. Development of active TB in persons with latent infection poses a continual threat of transmission. Dye C, et al. JAMA 1999;282:677 Transmission and Pathogenesis Transmission of M. tuberculosis • Spread by droplet nuclei • Expelled when person with infectious TB coughs, sneezes, speaks, or sings • Close contacts at highest risk of becoming infected • Transmission occurs from person with infectious TB disease (not latent TB infection) How contagious is TB? 10 secondary cases arise annually from 1 untreated smear-positive case. Index case Increased PPD + rate in household contacts (above age-matched control) Smear + 30%-50% Smear -/culture + 5% Smear -/culture - 0-8% ~50% of all TB cases are smear negative. Styblo K. Bull Int Union Tuberc 1978;53:53 How contagious is TB? Transmission is influenced by Number of AFB excreted from the source case (cavitary or laryngeal TB) Duration of exposure Closeness of exposure TB infection requires only 1-5 AFB deposited in terminal alveolus. TB Case Rates, United States, 2002 D.C. < 3.5 (year 2000 target) 3.6 - 5.2 > 5.2 (national average) Rate: cases per 100,000 25000 20000 15000 Year 1 9 0 9 7 9 5 1994 0 1990 9 3 9 1 9 9 8 5 7 8 1986 1998 2 1982 8 3 10000 8 No. of Cases Reported TB Cases United States, 1982-2002 2002 Epidemiology Recent increase in TB cases, including MDR-TB, in US (peak in 1992) Deteriorating public health infrastructure Inadequate institutional control of TB Urban crowding Epidemic of HIV Immigration After 1992, TB cases decrease in US. Cantwell MF, et al. JAMA 1994;272:535 Reported TB Cases by Age Group United States, 2002 <15 yrs (6%) 65+ yrs (21%) 45-64 yrs (28%) 15-24 yrs (10%) 25-44 yrs (35%) Reported TB Cases by Race/Ethnicity United States, 2002 Hispanic (27%) White, non-Hispanic (20%) American Indian/ Alaska Native (1%) Black, non-Hispanic (30%) Asian/Pacific Islander (22%) Number of TB Cases in U.S.-born vs. Foreign-born Persons United States, 1992-2002 20000 15000 10000 5000 0 1992 1994 1996 U.S.-born 1998 2000 Foreign-born 2002 Trends in TB Cases in Foreignborn Persons, United States, 1986-2002 No. of Cases Percentage 10,000 60 50 8,000 40 30 20 6,000 4,000 2,000 10 0 0 1986 1988 1990 1992 1994 1996 1998 2000 2002 No. of Cases Percentage of Total Cases Countries of Birth for Foreignborn Persons Reported with TB United States, 2002 Other Countries Mexico (25%) (38%) Philippines (11%) S. Korea Vietnam (3%) Haiti India (8%) (3%) China (5%) (7%) Length of U.S. Residence Prior to TB Diagnosis, United States, 2002 100% 80% 60% 40% 20% 0% All Philippines <1 yr 1- 4 yrs Mexico >5 yrs Vietnam Pediatric TB in USA Nelson LJ. Pediatr. 2004;114:333 Pediatric TB in USA In 2001, TB case rate in children <5 y: 2.8 per 100,000 5-9 y: 1.0 per 100,000 10-14 y: 0.9 per 100,000 Resist US-born Foreign-born INH 6.4% 10.9% MDR 1.4% 2.8% Nelson LJ. Pediatr. 2004;114:333 Testing for TB Disease and Infection Purpose of Targeted Testing • Find persons with LTBI who would benefit from treatment • Find persons with TB disease who would benefit from treatment • Groups that are not high risk for TB should not be tested routinely Risk-Assessment Questionnaires Place of birth Travel Exposure to TB cases Close contact with a person with +PPD Jail, shelter, illegal drug use, HIV Household members born/traveling outside US PPD is + in 6% of those with at least 1 risk factor vs 0.1% of those without any risk factors. Supplement to Pediatrics; Oct 2004 PPD Purified protein products from M. tuberculosis (5 TU) Stimulation of sensitized T-lymphocyte delayed-type hypersensitivity Response occurs at 2-10 weeks after TB infection Sensitivity 75-90% poor nutrition overwhelming acute illness immunosuppression Administering the Tuberculin Skin Test • Inject intradermally 0.1 ml of 5 TU PPD tuberculin • Produce wheal 6 mm to 10 mm in diameter (do not place control) • Do not recap, bend, or break needles, or remove needles from syringes • Follow universal precautions for infection control Reading the Tuberculin Skin Test • Read reaction 48-72 hours after injection • Measure only induration • Record reaction in millimeters PPD Ballpoint Pen Method Diameter of induration Classifying the Tuberculin Reaction 5 mm is classified as positive in • Recent contacts of known or suspected TB case • Persons clinical or radiographic findings consistent with active or previously active TB • Immunosuppressed patients: HIV Classifying the Tuberculin Reaction (cont.) 10 mm is classified as positive in Risk for disseminated disease • Concomitant medical conditions: DM, malnutrition, CRF, lymphoma • Those < 4 years old Risk for exposure to TB • • Born or travel to a country with high prevalence of TB Frequent exposure to cases with risk factors for TB • HIV, homeless, illegal drug use, immigrants Classifying the Tuberculin Reaction (cont.) 15 mm is classified as positive in • Persons with no known risk factors for TB • Targeted skin testing programs should only be conducted among high-risk groups PPD Cutoff value 5 mm immunocompromised host recent exposure to infectious case high probability of infection (abnormal CXR) 15 mm low risk of TB 10 mm others Factors that May Affect the Skin Test Reaction Type of Reaction False-positive False-negative Possible Cause Nontuberculous mycobacteria BCG vaccination Anergy Recent TB infection Very young age (< 6 months old) Live-virus vaccination Overwhelming TB disease Sensitivity of PPD: 80-96% Anergy • The use of control skin-test antigens has several limitations and IS NOT RECOMMENDED • It has not been standardized • The diagnosis of anergy has not been associated with high risk of developing TB Diagnosis of TB Evaluation for TB • Medical history • Physical examination • Mantoux tuberculin skin test • Chest radiograph • Bacteriologic or histologic exam “Clinical judgement” Tuberculosis is one of the great imitator. Common Sites of TB Disease • Lungs • Pleura • Central nervous system • Lymphatic system • Genitourinary systems • Bones and joints • Disseminated (miliary TB) Systemic Symptoms of TB • Fever • Chills • Night sweats • Appetite loss • Weight loss • Easy fatigability Conditions That Increase the Risk of Progression to TB Disease • • • • • • • • • HIV infection Substance abuse Recent infection Chest radiograph findings suggestive of previous TB Diabetes mellitus Immunosuppressed End-stage renal disease Chronic malabsorption syndromes Low body weight (10% or more below the ideal) Estimated HIV Coinfection in Persons Reported with TB United States, 1993-2001 % Coinfection 30 20 10 0 1993 1994 1995 1996 1997 1998 1999 2000 2001 All Ages Aged 25 - 44 Note: Minimum estimates based on reported HIV-positive status among all TB cases in the age group. All 2001 cases from California have an unknown HIV status. Chest Radiograph • • Abnormalities often seen in apical or posterior segments of upper lobe or superior segments of lower lobe Non-specific findings in children • May have unusual appearance in HIV-positive persons • Cannot confirm diagnosis of TB Arrow points to cavity in patient's right upper lobe. Specimen Collection • Obtain 3 sputum specimens for smear examination and culture • Persons unable to cough up sputum, induce sputum, bronchoscopy or gastric aspiration • Follow infection control precautions during specimen collection AFB smear AFB (shown in red) are tubercle bacilli Cultures • Use to confirm diagnosis of TB • Culture all specimens, even if smear negative • Results in 4 to 14 days when liquid medium systems used Colonies of M. tuberculosis growing on media Drug Susceptibility Testing • Drug susceptibility testing on initial M. tuberculosis isolate • Repeat for patients who - Do not respond to therapy - Have positive cultures despite 2 months of therapy • Promptly forward results to the health department Persons at Increased Risk for Drug Resistance • History of treatment with TB drugs • Contacts of persons with drug-resistant TB • Foreign-born persons from high prevalent drug resistant areas • Smears or cultures remain positive despite 2 months of TB treatment • Received inadequate treatment regimens for >2 weeks Data Collection and Analysis • TB reporting required in every state • All new cases and suspected cases promptly reported to health department • All drug susceptibility results sent to health department Treatment of Latent TB Infection (LTBI) Treatment of LTBI with Isoniazid (INH) • 9-month regimen considered optimal • Children should receive 9 months of therapy • Can be given twice-weekly if directly observed LTBI = PPD+ with normal H & P & CXR Treatment of LTBI with a Rifamycin and Pyrazinamide (PZA) HIV-Positive Persons • A rifamycin and PZA daily for 2 months • Administration of rifampin (RIF) contraindicated with some HIV drugs HIV-Negative Persons • Clinical trials have not been conducted • Daily RIF and PZA for 2 months • May be given twice weekly Contacts of INH-Resistant TB • Treatment with a rifamycin and PZA • If unable to tolerate PZA, 4-month regimen of daily RIF • HIV-positive persons: 2 month regimen with a rifamycin and PZA Contacts of Multidrug-Resistant TB • Use 2 drugs to which the infecting organism has demonstrated susceptibility • Treat for 6 months or observe without treatment (HIV-negative) • Treat HIV-positive persons for 12 months • Follow for 2 years regardless of treatment Monitoring Patients Baseline laboratory testing • Not routinely indicated • Baseline hepatic measurements for - Patients whose initial evaluation suggests a liver disorder - Patients with HIV infection - Pregnant women and those in immediate postpartum period - Patients with history of chronic liver disorder Treatment of TB Disease Basic Principles of Treatment • Provide safest, most effective therapy in shortest time • Multiple drugs to which the organisms are susceptible • Never add single drug to failing regimen • Ensure adherence to therapy Adherence • Nonadherence is a major problem in TB control • Use case management and directly observed therapy (DOT) to ensure patients complete treatment Directly Observed Therapy (DOT) High cure rate up to 95% even in resourcepoor countries Prevent additional spread Prevent development of drug resistance Cost-effective Directly Observed Therapy (DOT) • Health care worker watches patient swallow each dose of medication • Consider DOT for all patients • DOT should be used with all intermittent regimens • DOT can lead to reductions in relapse and acquired drug resistance • Use DOT with other measures to promote adherence 100% Mode of Treatment Administration in Persons Reported with TB United States, 1993-2000 80% 60% 40% 20% 0% 1993 1994 1995 DOT only 1996 1997 DOT + SA 1998 1999 SA only Directly observed therapy (DOT); Self-administered therapy (SA) 2000 Completion of TB Therapy United States, 1993-2000 100 * 80 60 40 20 0 1993 1994 1995 1996 1997 1998 1999 2000 Completed Completed in 1 yr or less *Healthy People 2010 target: Completed in 1 yr or less Note: Persons with initial isolate resistant to rifampin and children under 15 years old with meningeal, bone or joint, or miliary disease excluded. Treatment of TB for HIV-Negative Persons • Include four drugs in initial regimen - Isoniazid (INH) - Rifampin (RIF) - Pyrazinamide (PZA) - Ethambutol (EMB) or streptomycin (SM) • Adjust regimen when drug susceptibility results are Known (6 months) Extrapulmonary TB • In most cases, treat with same regimens used for pulmonary TB Bone and Joint TB, Miliary TB, or TB Meningitis in Children • Treat for a minimum of 12 months Treatment Regimens for TB Resistant Only to INH HIV-Negative Persons • Carefully supervise and manage treatment to avoid development of MDR TB • Discontinue INH and continue RIF, PZA, and EMB or SM for the entire 6 months • Or, treat with RIF and EMB for 12 months HIV-Positive Persons • Regimen should consist of a rifamycin, PZA, and EMB Multidrug-Resistant TB (MDR TB) • Presents difficult treatment problems • Treatment must be individualized • Clinicians unfamiliar with treatment of MDR TB should seek expert consultation • Always use DOT (or hospitalization) to ensure adherence Monitoring for Adverse Reactions • Baseline measurements • Monitor patients at least monthly • Monitoring for adverse reactions must be individualized • Instruct patients to immediately report adverse reactions Monitoring Response to Treatment • Monitor patients bacteriologically monthly until cultures convert to negative • After 3 months of therapy, if cultures are positive or symptoms do not resolve, reevaluate for - Potential drug-resistant disease - Nonadherence to drug regimen • If cultures do not convert to negative despite 3 months of therapy, consider initiating DOT Infection Control in Health Care Settings Infectiousness Patients should be considered infectious if they • Are coughing • Are undergoing cough-inducing or aerosol-generating procedures, or • Have sputum smears positive for acid-fast bacilli and they •Are not receiving therapy •Have just started therapy, or •Have poor clinical response to therapy Who should be placed in isolation? Most children with TB do not require isolation. Children with cough and Cavitary pulmonary TB Positive smears Laryngeal involvement Extensive pulmonary TB Adult household contacts (until proved not to have contagious TB) AAP Red Book 2000 How to isolate the patient? Transmitted by airborne droplet nuclei small particles < 5 µm which suspend in air for long periods Private room with negative-pressure ventilation Respirator mask Engineering Controls To prevent spread and reduce concentration of infectious droplet nuclei • Use ventilation systems in TB isolation rooms • Use HEPA filtration and ultraviolet irradiation with other infection control measures Personal Respiratory Protection Use in areas where increased risk of exposure: • TB isolation rooms • Rooms where cough-inducing procedures are done • Homes of infectious TB patients When does the patient become noncontagious? It is difficult to determine an absolute moment at which a pt on therapy becomes non-contagious. Discontinuation of isolation should be based on clinical improvement after appropriate treatment 3 negative smears collected on different days For MDR TB, need 3 negative cultures Multidrug Resistant Tuberculosis Red = hot spot Yellow = outbreak Multidrug-Resistant TB (MDR TB) Remains a Serious Public Health Concern • Resistance to INH 4% in 46 states and District of Columbia (DC) during 1993-1998 • 45 states and DC reported at least one MDR TB case during 1993-1998 Primary Anti-TB Drug Resistance United States, 1993-2002 % Resistant 10 5 0 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 Isoniazid MDR TB Note: Based on initial isolates from persons with no prior history of TB. MDR TB defined as resistance to at least isoniazid and rifampin. Percentage Primary Isoniazid Resistance in U.S.-born vs. Foreign-born Persons 14 United States, 1993-2002 12 10 8 6 4 2 0 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 U.S.-born Foreign-born Note: Based on initial isolates from persons with no prior history of TB. % Resistant Primary MDR TB in U.S.-born vs. Foreign-born Persons, United States, 19932002 3 2 1 0 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 U.S.-born Foreign-born Note: Based on initial isolates from persons with no prior history of TB. MDR TB defined as resistance to at least isoniazid and rifampin. When to suspect drug-resistant TB? Contacts of patient with drug-resistant TB Contacts of patient with prior treatment for TB Prior treatment for TB Persistent +AFB after 2-3 months of therapy Foreign-born Residents in area with high prevalence of drugresistant TB (INH resistance rate 4%) Take-home messages Always keep TB in differential diagnoses Aggressive work-up and treatment Use DOT Aggressive search for source and contact cases If in doubt, isolate the patient