Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sociality and disease transmission wikipedia , lookup
Infection control wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Germ theory of disease wikipedia , lookup
Periodontal disease wikipedia , lookup
Kawasaki disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Common cold wikipedia , lookup
Globalization and disease wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Rheumatoid arthritis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Behçet's disease wikipedia , lookup
Hepatitis B wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
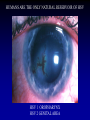
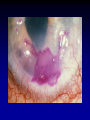
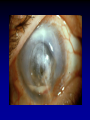
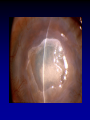
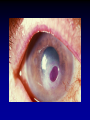
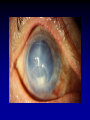
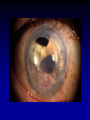
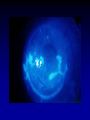
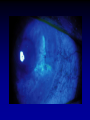
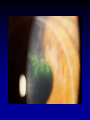
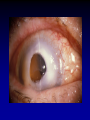
DIAGNOSIS AND TREATMENT OF HERPES SIMPLEX KERATITIS UPDATE XVI JORNADAS DE OFTALMOLOGIA DR. BENJAMIN BOYD AUGUST, 2005 RICHARD L. RICHARD L. ABBOTT, M.D. PROFESSOR OF OPHTHALMOLOGY UCSF FRANCIS I. PROCTOR FOUNDATION HUMANS ARE THE HUMANS ARE THE ONLY NATURAL RESERVOIR OF HSV HSV 1 OROPHARYNX HSV 2 GENITAL AREA TRIFLURIDINE VIDARABINE IDOXURIDINE HSV OCULAR DISEASE • • • • • • Approx. 1/2 million people in U.S. Approx. 20-45% of world population Approx. 50,000 active episodes annually Approx. 20,000 new cases annually By age 5….60% of population infected Only 6% develop clinical manifestations PRIMARY HERPES SIMPLEX • • • • • • • Acquired from environment (oral lesions, saliva) Not from viral latency Unilateral vesicular blepharoconjuntivitis Pruritic vessicles of lids, skin, eyelid margin Follicular conjunctivitis Palpable preauricular lymph node PEK (RARE dendrite) Look for vessicles Vessicles INFECTIOUS EPITHELIAL KERATITIS • • • • • Corneal vessicles (PEK) Dendrite Geographic (Amoeboid) ulcers Marginal ulcers (Limbal KC) May be associated with conjunctivitis TREATMENT Primary Herpes Simplex • Oral Acyclovir • Topical Trifluridine • Observation (self-limited) TYPICAL CORNEAL DENDRITE Of first importance in making the clinical diagnosis Dendron (Greek- “Tree”) True ulcer – extends through BM AVOID ROSE BENGAL IF CULTURE DDX: DENDRITIC KERATITIS • • • • • HSV HZV Healing epithelium Thimerosal (Toxicity) SCL HZV SOFT CONTACT LENS HEALING EPITHELIUM THIMERASOL TOXICITY HEALING EPITHELIUM HSV GEOGRAPHIC (AMOEBOID) ULCER • “Wide” dendrite • DDX epithelial defect – scalloped border • 4-20% of initial lesions • +/-Associated with previous steroid use LIMBAL (MARGINAL) HSV-I KERATITIS • Atypical presentation • More resistant to Rx • DDX: Staph marginal infiltrate – No epithelial defect – Progress circumferential – Associated with blepharitis – Typical location 2, 4, 8, 10 INCREASED INFLAMMATION WBC INFILTRATION TREATMENT Infectious Epithelial Keratitis • Goal: – Eliminate virus in short time • Purpose: – Decrease potential risk for immune-mediated disease – Decrease structural damage • Diagnosis: – Clinical, culture, PCR TREATMENT Infectious Epithelial Keratitis • Gentle debridement • Topical antivirals (10-14 days max) – Viroptic 1% q 2h or – Vira A 5X/day • If no response 72 hours – STOP • Resistance rate - 3% TREATMENT Infectious Epithelial Keratitis • If slow healing, consider toxicity • If epith ulcer persists, consider neurotrophic • Avoid steroids ACYCLOVIR REGIMEN • • • • • 400 mg 5x/day for 10-14 days Reduce to b.i.d. for 10 days Very safe Headaches, GI upset Watch dose renal disease HSV IRIDOCYCLITIS • 1-9% of all non-traumatic anterior uveitis • May occur independently • Live virus in aqueous • Average time to resolution: 4 weeks • Treat with topical steroids, cycloplegics, and PO Acyclovir • Watch IOP – Trabeculitis SECTOR IRIS ATROPHY • See in both Simplex and Zoster • Older patient - probably Zoster • If in doubt - treat with Zoster doses STROMAL KERATITIS • • • • • 2% of initial episodes 20-48% of recurrent HSV Disciform (Immune only) Necrotizing (direct viral invasion) Metaherpetic (post-herpetic trophic ulcer) IMMUNE (INTERSTITIAL) STROMAL KERATITIS (DISCIFORM) • Cell mediated immune response to viral antigens in stroma or endothelium DISCIFORM KERATITIS • • • • +/- Previous HSV epithelial keratitis Non-necrotizing Focal, multifocal, or diffuse area of edema Mild lymphocytic stromal inflammatory infiltrate- chronic and recurrent • Epithelium intact • Descemet’s folds and KP DISCIFORM KERATITIS • Differential diagnosis – HSV – HZV – Vaccinia – Mumps – Varicella STROMAL DISEASE • Treatment goals – Eradicate HSV – Limit scarring – Limit lipid deposition TREATMENT Stromal Keratitis • Treatment depends on severity and location of inflammation – Necrotizing keratitis – Interstitial keratitis – Immune rings – Limbal vasculitis – Disciform keratitis TREATMENT Disciform Keratitis • • • • Conservative - self limited Oral Acyclovir 400mg 5x/day Topical steroid - rapid taper No topical antiviral (poor penetration) NECROTIZING STROMAL KERATITIS • WBC’s (dense infiltrate with overlying defect • Blood vessels • Thinning • Scarring • Necrosis and perforation TREATMENT Necrotizing Stromal Keratitis • • • • • • Never studied by HEDS Acyclovir and topical steroids Taper slowly Maintain steroid at lowest dose Recurrence into visual axis Surgery STEROID TAPER • • • • • Pred Acetate qid > bid > qd > qod 4-6 weeks between steps Look for KP or edema Switch to weaker steroid Ask if redness when miss drop NEUROTROPIC KERATOPATHY POST HERPETIC EROSION (Metaherpetic Keratitis) • • • • Follows severe epithelial disease Basement membrane damage Non-healing epithelial defect Clinical course TREATMENT Neurotrophic Keratopathy • Goal: – Decrease exposure to toxic substances – Increase lubrication • Purpose: – Decrease risk 2º infection – Decrease risk of stromal melting • Diagnosis: – Rolled borders of epithelium TREATMENT Trophic Epithelial Defect • • • • • • Protect ocular surface Non preserved lubricants Therapeutic contact lens Gentle debridement Amniotic membrane Tarsorrhaphy ENDOTHELIITIS • Inflammatory reaction of endothelium • Corneal stromal edema without infiltrate (disciform, diffuse, linear) • KP, Stromal/epithelial edema, iritis • Responds to steroids REACTIVATION HSV • • • • • Hormonal changes Ultraviolet light Surgery of eye Systemic infection Latanoprost REACTIVATION HSV • • • • • • • • Stress Fever Immunosuppression Trauma (CL wear) 9.6% first year 36% @ 5 years 63% within 20 years HEDS: 18% recurrence rate RECURRENT HSV • Reactivation in latently infected cells • Disease pattern affected by: – Strain of virus (Can block subsequent infection by another strain) – Genetic constitution of host PROPHYLAXIS FOR HSV KERATOPLASTY • Use oral acyclovir – Pre-op: – Post-op: 400mg qid for 3 days 400mg qid for 7 days 400mg bid for 3months • No controlled studies available TREATMENT Stromal Keratitis • If corneal perforation: – Surgical adhesive – Lamellar patch graft – PKP Use of oral Acyclovir VALACYCLOVIR (Valtrex) • Absorbed rapidly from GI tract • Converted into Acyclovir (Prodrug) • Plasma levels 3 times higher than same dose with Acyclovir • Do Not Use with renal disease and HIV • Dose: 1 Gram qd FAMCICLOVIR • • • • MOA similar to Acyclovir Inhibits HSV DNA synthesis Rapidly absorbed from GI tract Intracellular 1/2 life is 10-20 times longer • Lactose intolerance FAMCICLOVIR • Dose: 500mg bid-tid • Side effects similar to Acyclovir • More expensive cost CIDOFOVIR PENCICLOVIR • Variation in chemical structure • Inhibit DNA polymerase • Less resistance VALTREX AND FAMVIR • Not more effective than Acyclovir • Cost issue • Compliance issue HEDS STUDY RESULTS • Oral antiviral prophylaxis reduces recurrences of epithelial and of stromal keratitis • Use of topical steroids is of benefit in stromal keratitis • Use of oral acyclovir may be of help in iridocyclitis • Prophylactic oral acyclovir helps prevent recurrences of herpetic keratitis, particularly stromal with a history of recurrence