Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Molecular mimicry wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Vaccination wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Common cold wikipedia , lookup
Hepatitis B wikipedia , lookup
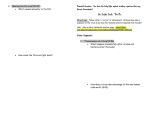
The Threat of Influenza Damara Gebauer Sai Jahann Bonnie Hart Influenza • • • • Overview Molecular Biology Clinical Bioweaponization Influenza Overview • Commonly called “the flu”. It is a highly contagious disease caused by the influenza virus. • It is a disease of the respiratory system, namely the throat, nose and lungs. • Can affect people of all ages including healthy people and symptoms are seen suddenly. Influenza Overview • People most susceptible are the elderly, small children and immuno-compromised, although anyone can develop complications. • Complications include pneumonia, bronchitis, nose and ear infection. • “Stomach Flu” Myth • No aspirin for children or teenagers Influenza Overview • 10-20% of the US population come down with the flu each year. • ~36,000 Americans succumb to complications of the disease. 250,000 people die world wide. • Vaccines are the first line of defense. • Antiviral medication is also available • Viral receptor proteins are primary targets of vaccines and antivirals • Hemagglutinin (HA) and Neuraminidase (NA) are targeted viral proteins Influenza Strains • Single negative-stranded RNA virus • 3 Types: A, B, C http://web.uct.ac.za/depts/mmi/stannard/fluvirus.html Influenza Strains Type Natural Reservoir Animals affected Disease Epidemic in Humans A waterfowl humans, pigs, chickens flu and flu complications yes B unknown mostly humans only flu and flu complications yes C unknown humans mild respiratory illness no Type A www.omedon.co.uk/.../beans/ influenza%20virus.jpg Beware of Type A • 15 known HA subtypes: H1-H15 • 9 known NA subtypes: N1-N9 • While all subtypes can be found in birds, only H1H3 and N1-N2 are known to circulate widely in humans. • H1-H3 are the only types known to have caused pandemics in humans – Pandemics arise from flu strains that have novel HA and NA proteins that people have no immunity to Beware of Type A • New strains can form by genetic re-assortment between animal and human strains. 1956 (Asian) and 1968 (Hong Kong) were formed this way. • Recently been discovered that wholly avian strains CAN directly infect humans • Epidemic occurred in 1997 in Hong Kong. 18 people were infected and 6 died from complications. Beware of Type A • Previously it was thought that humans could not be infected by wholly avian flu and that an intermediary step was required • Pigs were thought to be this intermediary step. • Avian or some other animal flu infected pigs, reassortment occurs creating new strain which then has potential to infect humans. • 1997 Hong Kong incident showed pigs are not required to be intermediary step since reassortment can occur directly in humans Avian flu: Why such a threat? • HA and NA surface proteins are generally not recognized by human respiratory cells • Wholly avian flu infects humans at a low frequency but has huge pandemic potential. • 1997 Hong Kong incident was first case of wholly avian flu infecting humans. Fortunately, flu could not spread from person to person. Avian flu: Why such a threat? • If avian strain were to spread from person to person, most of the population will have no prior immunity to the HA and NA proteins and a devastating pandemic could occur. • Also, if avian strain and common human strain infect host simultaneously, could get re-assortment and creation of a super influenza strain. • WHO and other organizations are watching Asia and other countries with avian flu outbreaks very closely Three Pandemics in 20th Century • 1918 Spanish Influenza– A(H1N1) • 1957Asian Influenza—A(H2N2) • 1968 Hong Kong Influenza—A(H3N2) Spanish 1918 Pandemic Influenza A H1N1 http://www.stanford.edu/group/virus/uda/ Spanish Influenza 1918 • The most devastating flu pandemic the world had seen. • Named Spanish influenza because of the severe loss in Spain. 8 million people died in May 1918. • In the U.S, first signs were seen in early spring in military camps in Kansas, but received little attention because of the war in Europe. Spanish Influenza 1918 • By the fall, hospitals were overwhelmed with patients, many of whom were dying 23 days after exhibiting symptoms. • The pandemic was extremely sudden. No one was prepared. In the US, the average life span was reduced by 10 years. • ~675,000 American deaths. Spanish Influenza 1918 • 40 million people worldwide were dead from the flu. • Most striking was the high morbidity of young people (20-40 years old). • Influenza's full impact: millions of hospitalizations, secondary bacterial pneumonias, and middle ear infections in infants and young children. • Caused by H1N1 strain that resembled most closely swine origin. 1957 Asian Influenza—A(H2N2) • Re-assortment of avian and human strains. • Re-assortment thought to have occurred in pigs. • 70,000 deaths in America. First identified in China in February 1957, it spread to the US by June 1957 1968 Hong Kong Influenza—A(H3N2) • Also re-assortment of avian and human strains. • 34,000 deaths in America. Started in Hong Kong in early 1968 and spread to America by the end of the year. • A(H3N2) is still circulating in human population today. Influenza Today • Kills an average of 36,000 Americans every year and 250,000 around the world. • ~115,000 Americans are hospitalized for the flu each year http://www.nlm.nih.gov/medlineplus/news/fullstory_16132.html Recent News: Revenge of the Birds • 1997 Hong Kong A(H5N1)- First reported case of direct transmission from bird to human. • 1999 Hong Kong A(H9N2)- 2 children infected with avian flu and transmission was believed to be direct bird to human. Both children recuperated. • 2003 Hong Kong A(H5N1)- a father and son traveling to mainland came down with flu, father did not survive. Source of infection remains unknown. Recent News • 2003 Netherlands A(H7N7)- Outbreak of avian flu in farmed poultry. 80 poultry workers and their families became ill. There seemed to be some human to human transmission. One patient died. • 2003 Hong Kong A(H9N2)- One child became ill with avian flu but recovered. • Present day- Several Asian countries including China, Thailand, Vietnam, Indonesia and others are having outbreaks of avian flu among farmed poultry. Influenza: Molecular Biology • What differentiates influenza from other viruses? • How does an influenza virus particle interact with a host cell? • Why is it so contagious? So dangerous? Characteristics of viruses • • • • Genome enclosed in protein shell Can only reproduce within host cell Each type of virus has specific “host range” Reprogramming of cell – Copy viral genes – Manufacture viral proteins Structure of Influenza • Viral envelope – Surface studded with spikes • Matrix protein (M1) • 8 RNA segments • Non-structural proteins – – – – Nuclear export protein (NEP) NS1 protein Nucleocapsid protein (NP) Polymerase components Surface proteins of influenza A/B • Hemagglutinin (HA) – Rod-shaped – Binds virus to host cell to initiate infection – Brings about fusion – 15 types • Neuraminidase (NA) – Mushroom-shaped – Prevents viral aggregation upon release – 9 types Genome segments of influenza A Genome segments – encoding • • • • • 4: HA 6: NA 7: M1/M2 Matrix proteins 5: Nucleoprotein (NP) 1,2,3: Polymerase machinery (PB-2, PB-1, PA) • 8: Non-structural proteins: NS1, NEP Genetic variation of influenza A • Causes introduction of new, pandemic strains • Mutational frequency comparable to other viruses – Can’t be the only explanation • Unique ability to undergo antigenic variation – Antigen: interacts with cell and antibody – Antigenic drift: minor changes – Antigenic shift: major differences; new strains Genetic Variation: Antigenic Drift • Accumulation of point mutations eventually result in amino acid substitutions • HA glycoprotein: – Results in differences in key antigenic sites at which the host antibody binds – Prevent binding of antibodies induced by previous infection • Also occurs in NA glycoprotein Genetic Variation: Antigenic Shift • Involves replacement of entire gene segments – Results in novel viruses • Occurs suddenly in association with pandemics • Through dual infection: different influenza viruses infect a single cell • Does not occur in NA glycoprotein Genetic Variation: Antigenic Shift • One cell is infected by two different influenza A viruses – Not necessarily human flu • Inside the cell, spontaneous self-assembly can produce recombinant viruses • Those viruses bud out of cell and infect other host cells • A new flu strain is born! Infection cycle of influenza 1. 2. 3. 4. 5. 6. 7. Binding of virus to cell Cell engulfs virus via endocytosis Membrane of virus fuses with endosome; RNA released into cell Viral polymerase produces mRNA from viral RNA Protein, new RNA produced Self-assembly produces virions Virions bud off cell membrane Infection cycle: Binding and endocytosis • HA contains receptor binding site for virus – Binds to sialic acid residue on cell surface glycoprotein • Binding triggers receptormediated endocytosis – Virus is taken into endosome – Low pH of endosome causes fusion of viral and endosome membranes Infection cycle: Endocytosis and membrane fusion Infection cycle: Fusion of viral and cell membranes • Cleavage of HA is necessary – This allows fusion of membranes • HA cleaved at arginine in cleavage site • More arginines = more proteases cleaving – Mutated viruses can be cleaved by more proteases • Virus is more infective – More of the cells it attaches to will get exposed to viral genome. Infection cycle: Viral replication • Negative-sense viral RNA is transcribed to mRNA by viral polymerase (PB1, PB2, PA) – mRNA complements made for incorporation into new virions – mRNA translated to produce viral proteins • For incorporation into virions • For use in infected cell (NEP, NS1) Infection cycle: Viral budding • HA and NA incorporated into host cell membrane • M1 matrix protein forms shell, bound to: – Cytoplasmic tails of HA, NA – Viral ribonucleoproteins – Other M1 molecules • Virus buds off via exocytosis Host cell v. influenza A virus • Human cell has initial antiviral defenses – Interferon-α/β-independent response – Protein kinase R – Interferon-α/β response • Virus needs to counteract these to reproduce – NS1A protein Host cell v. influenza A virus • Interferon-α/β-independent protection – Upon infection by virus, activate transcription factors that control expression of antiviral genes • Interferon regulatory factor-3 (IRF-3), IRF-7 • Combine with coactivators to form virus-activated factor (VAF) • VAF induces transcription of genes that code for antiviral proteins Host cell v. influenza A virus • Protein Kinase-R (PKR) protection – Activated by presence of double-stranded RNA • Consequence of RNA virus presence in cell – Activated PKR inhibits protein synthesis and therefore viral replication • Phosphorylates translation initiation factor eIF2 Host cell v. influenza A virus • Interferon-α/β response – Infected cell produces IFN-α/β • Signal travels to neighboring uninfected cells – In infected and neighboring cells, induces transcription of antiviral proteins • Protects infected cell against current infection • Prepares at-risk cells to withstand infection – Induces production of MxA protein • Largely responsible for inhibition of influenza A Host cell v. influenza A virus • Influenza NS1A protein inhibits 3’-end processing of cell mRNA – Prevents addition of poly-A tail – Doesn’t affect viral mRNA processing • Inhibits activation of PKR – Mechanism not clearly understood • Enough IFN-β produced to protect neighboring cells Influenza effect on host cells • Turns off protein function – NS1A protein • Causes cell death – Induces apoptosis – Dead cells shed off respiratory tract lining – Can cause shedding down to basement membrane layer • Infects respiratory tract; causes clinical symptoms Flu-Clinical Influenza Virus Types • Type A – humans and other animals – all age groups – moderate to severe illness • Type B – milder epidemics – humans only – primarily affects children • Type C - uncommon strain, no epidemic Common Flu Symptoms • High Fever • Headache • Extremetiredness/weakness • Dry cough • Sore throat • Stuffy/runny nose • Muscle aches • Diarrhea and vomiting Cold v. Flu • Flu is worse than common cold • Symptoms more intense in flu (fever, body aches, tiredness, and dry cough) • Colds- more likely to have runny or stuffy nose • Colds don’t result in serious health problems (pneumonia, bacterial infections, or hospitalizations) Increased Risk • • • • Age 65 and older Any age with chronic medical conditions Pregnant women Children 6-23 months Emergency Warning Signs- In children • • • • • • • High or prolonged fever Fast breathing or trouble breathing Bluish skin color Not drinking enough fluids Changes in mental status Flu-like symptoms improve but then return Worsening of underlying chronic medical conditions Emergency Warning Signs- In adults • • • • • • High or prolonged fever Difficulty breathing or shortness of breath Pain or pressure in chest Near-fainting or fainting Confusion Severe or persistent vomiting Peak Months for Flu Activity (over the past 21 years) 40 35 30 25 20 15 10 5 0 Dec Jan Feb Mar Apr May How the Flu Spreads Spread of Flu • Droplet Spread – from a person’s cough or sneeze – person touches respiratory droplets on another person or object and then touches their own mouth or nose • Incubation period = 1-4 days (avg. = 2 days) • Adults infectious from day before symptoms begin to 5 days after illness onset • Children- infectious for > 10 days Symptoms • Adults- shed virus 1 day before developing symptoms to 7 days after getting sick • Young children- can shed virus for longer than 7 days Complications • Bacterial pneumonia • Dehydration • Worsening chronic conditions – congestive heart failure – asthma – diabetes • Children can develop sinus problems and ear infections Complications-cont. • Lead to pulmonary or cardiac disease • Lead to 2ndary bacterial pneumonia or primary influenza viral pneumonia • Children – 20% hospitalized can have febrile seizures • Influenza is associated w/ encephalopathy, transverse myelitis, Reye syndrome, myositis, myocarditis, and pericarditis Influenza and Complications Among Nursing Home Residents 9 8 7 6 5 Vaccinated Unvaccinated 4 3 2 1 0 Hosp Pneu Death Hospitalization from Influenza • Highest rate among young children and persons >65 yrs • 1969-70 through 1994-95 influenza epidemic: 16,000-220,000 hosp./epidemic • 114,000 hospitalizations/yr with 57% occurring in ages < 65 yrs • Highest # caused by type A (H3N2) viruses Deaths • Result from pneumonia and/or worsening of cardiopulmonary conditions and other chronic diseases • 5th leading cause of death for adults > 65 • 1976-90 epidemic 19,000 deaths • 1990-99 epidemic 36,000 deaths • In 23 epidemics (‘72-’95): 20,000 excess deaths in 11 epidemics and 40,000 deaths in 6 epidemics Death rates from influenza-associated pulmonary and circulation deaths/100,000 persons • • • • 0-44 yr: 0.4 - 0.6 50-64yr: 7.5 65yrs: 98.3 Reasons: – more older people has inc. – Influenza A associated with higher mortality – Influenza A predominates in 90% of seasons from 1990-99 compared w/57% of seasons 1976-90 Laboratory Diagnosis • Can determine circulating types, subtypes, and strains • Tests include – – – – – viral culture serology rapid antigen testing PCR immunofluorescence Commercial rapid diagnosis tests • Detect viruses in 30 minutes • Specimens used are either throat swabs, nasal wash or nasal swab • Sensitivity of rapid tests are lower than that of viral cultures confirm (-) tests with viral culture • Does not provide specific info on circulating subtypes and strains Preventing the Flu • Good Health Habits • Vaccination • Antiviral Medications Good Health Habits • Avoid close contact • Stay home when you are sick • Cover your mouth • Clean your hand • Avoid touching your eyes, nose or mouth • Get plenty of rest • Drink plenty of liquids • The simplest way to avoid the flu is to avoid crowds. Can’t keep you kids cooped up? Frequent hand washing is the next best thing Vaccination Vaccination • Best way to prevent flu • Selection of virus for manufactured vaccine made in Feb and April each year • Get vaccinated each fall • People at high risk should get vaccinated • 2 kinds of vaccines – inactivated – live attenuates (LAIV) (for ages 5 - 49) Who Should Not Get Vaccine • Have severe allergy to hen’s eggs (anaphylactic allergic rxn) • People who previously developed GuillianBarre syndrome (GBS) w/in 6 weeks after getting a flu shot Live Attentuated Intranasal Influenza (LAIV) • Contains weakened live influenza vs killed viruses • Administered by nasal spray • Contains 3 different live (but weakened) viruses, which stimulate body to make antibodies Live Attentuated Intranasal Influenza (LAIV) • Attenuated, producing mild or no signs or symptoms • Temperature-sensitive-limits the replication of vaccine viruses at 38-39°C restricts LAIV viruses from replicating efficiently in human lower airways • Cold-adapted, replicating efficiently at 25°C restrictive for replication of different wild-type viruses Dosage-LAIV • 0.5 mL of vaccine: 0.25 mL for each nostril • Children aged 5-8 previously unvaccinated: receive 2 doses separated by 6-10 weeks • Children aged 5-8 previously vaccinated: receive 1 dose (do not require a 2nd dose) • Persons aged 9-49: receive 1 dose Efficacy & Effectiveness of LAIVchildren • Season 1: – 93% efficiency for those who received 2 doses – 91% for those those who received 1 dose • Season 2: – 86% overall efficiency – A (H2N2) component of vaccine was not well matched for circulating virus strains Efficacy & Effectiveness of LAIVadults • 85% overall efficiency • Vaccination reduced severe febrile illnesses by 19% and upper respiratory tract illnesses by 24% • Fewer days of illness • 15-42% fewer health care provider visits • 43-47% less use of antibiotics LIAV Side Effects • Children – – – – – runny nose headache vomiting muscle aches fever • Adults – – – – – runny nose headache sore throat cough fever Inactivated Influenza Vaccine • Contains two type A and one type B • Made from purified, egg grown viruses that have been inactivated or killed • Antibiotics can be added to prevent bacterial contamination • Vaccinated people develop high postvaccination hemagglutination inhibition antibody titers Dosage-Inactivated • 15g/dose of H1N1 virus and H3N2 type A virus plus a type B strain • Children previously unvaccinated: 2 doses one month apart (2nd dose should be administered before December) • Vaccinated in the deltoid muscle ( needle length > 1 inch in order to penetrate muscle tissue in adults;7/8-1 inch for children) • Infants should be vaccinated in the anterolateral aspect of the thigh Effectiveness of Inactivated Vaccine- Children • 77% - 91% effective against influenza respiratory illness • Effective against influenza seroconversion: – age 1-5 – age 6-10 – age 11-15 44- 49% 74-76% 70- 80% • Another study: > 89% overall efficiency for 6-24 months old Effectiveness of Inactivated Vaccine-Adults • Aged < 65 yrs old: – 70-90% efficient – work absenteeism, health-care resources • Aged > 65 yrs old: – 50-60% effective in preventing hospitalization for pneumonia and influenza – 80% effective in preventing death Side Effects to Inactivated Vaccine • Soreness at vaccination site • Fever, malaise, myalgia • Guillain Barre Syndrome: 1 additional case per 1 million people – Body's immune system attacks part of the nervous system and results in weakness or tingling sensations in the legs that can spread to the arms and upper body. – Can result in paralysis Inactivated v. Live Vaccines • Similarities – contain one influenza A (H3N2) virus, one A (H1N1) virus, and one B virus – vaccines grown in eggs – administered annually • Differences – Inactivated has killed virus, LAIV contains attentuated viruses – Cost: LAIV more expensive – who gets what vaccine – Administration • LAIV: intranasally • dead: intermuscularly Antiviral Medications • 4 medications: – Amantadine: orally administered, treats type A – Rimantadine: orally administered, treats type A only for adults – Oseltamivir-capsule, treats type A & type B – Zanamiv-inhaled powered drug, treats type A& type B • Last for 5 days and must be started w/in the 1st 2 days of illness • Used to control outbreaks in institutions Antiviral Medications • Drugs are 70-90% effective for prevention • If taken w/in 2 days of getting sick, drugs reduce symptoms and shorten time of sickness by 1-2 days • Have side effects Amantadine and Rimantadine Side Effects • CNS side effects: nervousness, anxiety, difficulty concentrating, light headedness (occur more often w/amantadine) • Gastrointestinal side effects: nausea, loss of appetite • People w/ long-term illnesses: delirium, hallucinations, agitation, and seizures • Side effects disappear after 1 week Zanamivir Side Effects • Drug is inhaled and can effect those w/asthma or other chronic lung diseases • Decreased respiratory function, bronchospasm • Less than 5% reported diarrhea, nausea, sinusitis, nasal infection, bronchitis, cough, headache, and dizziness Oseltamivir Side Effects • Gastrointestinal side effects – nausea – vomiting • Less severe if taken with food Economics • Annual direct medical cost = $4.6 billion • Total direct and indirect costs = $12 billion (indirect includes work days lost, school days lost, etc.) • Vaccination can reduce these costs from hospitalizations, lost work days and antibiotic use. Is a pandemic imminent? • Experts (WHO, CDC) are saying yes. • It will occur as a natural disaster or as a bioterrorist attack. • Either way we are not ready to respond to a flu pandemic Influenza as a Bioweapon? 1. Suicide bio-bomber:a terrorist infects himself with super flu (e.g. avian and human influenza cross), spreads infection. 2. Now possible to make infectious flu virus from cloned DNA of the 8 RNA segments. This could bring back the 1918 Spanish Influenza. 3. Genetically modify avian flu strain so that can recognize human hosts’ receptors. This could be deadly. Bioweapon Pros • Highly contagious • Difficult to contain people (as opposed to animals) • Hard to determine strain for vaccine defense • Mostly likely will not have appropriate vaccine(s) at time of attack. • Relatively easy to obtain. Bioweapon Pros • Infect farmed poultry and damage poultry industry and the US economically. • Flu strain need not be lethal since it’s so contagious already. If infect enough people can cause social and economic strain by wiping out work force. • First cluster of cases would probably not alert officials. This could give pandemic head start. • Difficult to eradicate because of bird and other animal reservoirs. Bioweapon Pros • Greater threat to world leaders because they are generally older and more susceptible to the virus. Bioweapon Cons • Strain may not be lethal, people could recuperate • So far, wholly avian strain can not get human to human transmission. This would not be contagious. • Highly unlikely that terrorists would have expertise to conduct recombinant DNA technology research or have the resources. Lines of Defense • Stockpiles of vaccines, may have to replenish to account for strain shifts • Increase security and monitor laboratories conducting influenza research and manufacturers that are distributing vaccines and antivirals. • Healthcare workers should increase immunization for people who need it now. • Equip healthcare workers and possibly pharmacies with proper flu assay kits so they can identify disease quickly. Therefore, Beware! • Influenza is more than “just a cold” • A pandemic can have drastic social, economic, and health consequences • Influenza is a potential and effective bioweapon that we should be prepared to see