Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
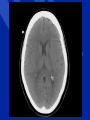
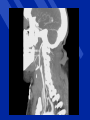
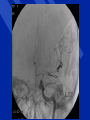
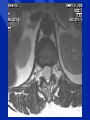
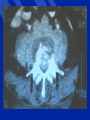
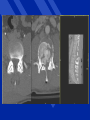
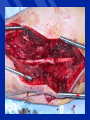
Back to Basics for Surgery Neurosurgery R. Moulton Principles of Neurological Diagnosis Questions What is the lesion Where is the lesion History Physical (Neurological) Examination Special Tests Presentation of Neurosurgical Illness Raised ICP – Headache, vomiting – papilloedema Neurological Dysfunction – General – level of consciousness – Focal – sensory or motor loss Seizures Pain What is the lesion – history Where is the lesion – neurological exam History (What is the lesion?) Symptoms Mode of onset Speed of onset Prior relevant illness Progression/regression of symptoms Neurological Examination (Where is the Lesion?) Level of Consciousness – GCS Mental status – orientation, memory, concentration, abstraction, calculation Cranial Nerves Motor examination – Upper vs. lower motor neuron – Cerebellar function – Gait Sensory examination – light touch, pain & temp, joint position sense – Cortical sensory modalities Cranial Nerves I Olfactory II Optic III Oculomotor IV Trochlear V Trigeminal VI Abducens VII Facial VIII Acoustic IX Glossopharyngeal X Vagus XI Accessory XII Hypoglossal Motor Examination Upper Motor Neuron – Weakness (distal > proximal) antigravity muscles preserved – Increased reflexes and tone (spasticity) – Disuse atrophy – Loss of coordination (ataxia) – Apraxia – Upgoing plantar response Lower Motor Neuron – – – – – Weakness Decreased tone Decreased reflexes Denervation atrophy Coordination usually intact Sensory Examination Special senses – cranial nerves Basic Modalities – Light touch, pain & temp, vibration & proprioception – Dermatomes, peripheral nerve distribution Cortical Modalities – Graphaesthesia, stereognosis, simultaneous appreciation of tactile stimuli, somatotopognosis, agnosagnosia, neglect Special Tests Biochemical, hematological, microbiology – Blood – CSF Imaging – – – – Plain x-rays CT MRI Angiography Electrophysiology – EMG, nerve conduction, EEG etc. Neurological Examination of the Comatose Patient Level of Consciousness – Glasgow Coma Score Brainstem Integrity – – – – Pupillary Reaction Ocular Movement Corneal reflexes Gag/breathing Eye Opening spontaneous to voice to pain none Verbal Response oriented confused - sentences words only sounds none 4 3 2 1 5 4 3 2 1 Movement obeys localises flexion withdrawal abnormal flexion extension none 6 5 4 3 2 1 Rostral-Caudal Deterioration Midbrain – Bilateral pupillary abnormalities – Oculomotor abnormalities Pons – Loss of corneal reflexes Medulla – Loss of gag reflexes – Respiratory and vasomotor collapse Brain Tumour Classification Intra-axial (frequently malignant) Primary – – – – – – – Glial Choroid plexus Neuronal or mixed glial-neuronal PNET/medulloblastoma CNS lymphoma Pineal region hemangioblastoma Metastatic Brain Tumour Classification Extra-axial (usually benign) – – – – Meninges Cranial nerves (Schwannoma) Pituitary skull Glial Tumours Astrocytoma (gliobastoma multiforme) Oligodendroglioma Ependymoma Mixed tumours Gr. I - IV Treatment Supportive Specific – Corticosteroids (dexamethasone) – Surgical » Biopsy » Excision » Internal decompression Treatment contd. – Radiotherapy » Conventional » Stereotactic focused – Chemotherapy » Temazolamide (malignant glial tumours) » Lymphoma protocols » Specific to tissue of origin for metastases Observation No Contrast With Contrast Stroke: Classification and Management Stroke Definition Sudden onset of a neurological deficit due to disease or injury of the blood supply of the brain. Stroke Classification Ischemic – Bland – Hemorrhagic transformation Hemorrhagic (hemorrhage is 10 event) – – – – – Hypertension Amyloid angiopathy Aneurysmal AVM Other Ischemic Stroke (Infarction) Thrombotic (local vessel disease) Embolic – – – – Artery to artery (usually carotid) Heart to artery (atrial fibrillation) Paradoxical (vein to artery) Other (air, foreign body, iatrogenic) Intracerebral Hemorrhage Hypertensive – Occurs in long narrow perforating arteries (basal ganglia, thalamus, pons, cerebellar nuclei) – Charcot-Bouchard aneurysms – Related primarily to duration of hypertension Intracerebral Hemorrhage Amyloid angiopathy – Age related change in cerebral vessels – Lobar hemorrhage – Most commonly in posterior part of cerebral hemispheres Intracerebral Hemorrhage AVM Berry aneurysm Subarachnoid hemorrhage – Usually exclusively subarachnoid – May have intracerebral component – Occasionally exclusively intracerebral Management Diagnosis – History – Physical Examination – Special tests (imaging) Treatment Stroke Diagnosis History – Rapid onset fixed deficit – ischemic – Rapid onset progressive deficit – hemorrhage – Sudden severe headache, nausea/vomiting/photophobia +/neurological deficit - SAH Stroke Physical Examination Focal deficits – Most often ischemic stroke or ICH – Much less common in SAH Alteration in level of consciousness – SAH – ICH – Delayed swelling from large infarcts Stroke Investigation CT scan – First line imaging to distinguish infarct from hemorrhage – 1st choice for confirming SAH, LP if negative Other – Cerebral angiography, doppler for carotids – MRI in special circumstances Acute Stroke Treatment Supportive – Airway – Blood pressure Definitive – Thrombolysis – Hematoma evacuation (limited circumstances) Stroke Treatment Prevention – Risk factor modification » Hypertension, smoking, diabetes, lipids/cholesterol – Antiplatelet agents (artery-artery embolism, local occlusive disease) – Anticoagulation (heart to artery emboli) – Surgical prevention » Carotid endarterectomy, stenting » Aneurysm obliteration » AVM excision Skull Fracture Primary Impact Injury Shear (diffuse) injury of axons Laceration/contusion of cortical surface Blumbergs, Head Injury, 1997:45 Cerebral Contusions Secondary Insults Hypoxia Ischaemia Intracranial hematomas Raised intracranial pressure Seizures Infection Fluid and electrolyte disturbance Respiratory Changes in Head Injury Depression/abolition of gag and cough reflexes Hypercarbia 2o to respiratory centre depression Hypoxemia -- systemic causes – inadequate airway management – chest trauma – aspiration Recommendations for Treatment Resuscitate aggressively with appropriate fluid Brain oedema is not a concern Manage source of bleeding in unstable patients prior to transfer Do not use mannitol in presence of hypotension or you will further destabilise the patient Consider transient use of vasopressor drugs while restoring volume and controlling haemorrhage Trauma Craniotomy Incision Pressure Volume Curve Pressure Vskull = Vbrain + Vblood + VCSF + Vmass Volume Trans-Tentorial Herniation Use of Mannitol .5 - 1 gm./kg of 20% solution give as a bolus urinary catheter Contraindications: Shock Anuria Other ICP Therapies CPP therapy Barbiturate Coma Decompressive Craniectomy Back to Basics For Surgery Spine Pain Generators Myofascial Disc Facet Joint Nerve Visceral Vascular Physical Examination: The Spine Inspect: deformity Palpate: deformity, local tenderness Range of motion (limitation, pain) Myelopathy ‘a general term denoting functional disturbance and/or pathological changes in the spinal cord’ Myelopathy Important Questions Level of lesion Nature of lesion – Surgical (spondylotic, neoplastic, infectious, hematoma, traumatic) – Treatment frequently curative – Non-surgical (degenerative, inflammatory) Degree of patient disability Rate of progression History, physical examination, special investigations Myelopathy: History Patient Complaints: Numbness (loss of sensation, alteration of sensation – paraesthesia, awkwardness) Ataxia (awkwardness, clumsiness) – Usually: – Gait (imbalance, unsteadiness, unable to move quickly) – Fine movements of hands (doing up buttons, handwriting) Weakness – usually a late finding Myelopathy: History Patient Complaints: Numbness (loss of sensation, alteration of sensation – paraesthesia, awkwardness) Ataxia (awkwardness, clumsiness) – Usually: – Gait (imbalance, unsteadiness, unable to move quickly) – Fine movements of hands (doing up buttons, handwriting) Weakness – usually a late finding Myelopathy: History Limbs involved: lower (may be thoracic or cervical), upper and lower (always cervical) Onset: gradual, rapid or sudden Associated pain: – Activity related: spondylotic – Nocturnal: neoplastic – Associated radicular pain Previous or concurrent neurological symptoms/illness Myelopathy: Physical Examination Motor: – Strength: weakness is usually late finding in slowly evolving surgical conditions, occurs in corticospinal distribution – Reflexes (change occurs early): hyperactive distal to lesion in gradually evolving lesions » In disc disease may be hypoactive at level of lesion Myelopathy: Physical Examination – Tone (early): increased distal to lesion – Coordination (early): impaired distal to lesion – Plantar responses: up-going (reliability?) Sensation: – Proprioception: frequently impaired in lower limbs – impossible to establish precise level – Pinprick: extremely useful in thoracic lesions Special Investigations Plain x-rays (bone destruction, fracture, subluxation, spondylotic changes), n.b. no visualization of nervous tissue CT scan (same indications/contraindications as x-ray) MRI usually the definitive investigation CT-myelography (most useful for looking at bone and disc relation to spinal cord/nerve roots) Myelopathy: Surgical DecisionMaking Nature of the lesion Natural history of the lesion – Trauma: static/improving unless spine unstable – Neoplastic: progressive, rate variable depending on histology – Infectious: usually rapidly progressive – Spondylotic myelopathy, usually gradually progressive, rate variable – Recovery usually poor with advanced deficits Myelopathy: Surgical Approach Lesion site: – Extradural – Intra-dural, extra-medullary – Intramedullary Extradural: – Anterior pathology – anterior approach – Posterior pathology – posterior approach (laminectomy) Intradural-extramedullary – posterior Intradural-intramedullary - posterior Radiculopathy a general term denoting functional disturbance and/or pathological changes in a spinal nerve root Radiculopathy Symptoms – Pain, paraesthesiae, sensory loss in the approximate dermatome of the involved nerve root – Axial pain is not a symptom of nerve root involvement – Weakness in the myotome of the involved nerve root – pts. frequently can’t be specific Radiculopathy Exam findings – Lower motor neuron findings in the appropriate myotome – Sensory findings in the appropriate dermatome Radiculopathy – Investigation Lumbar – MRI, CT scan Cervical/thoracic – MRI Radiculopathy - Conservative Tx Activity modification NSAIDS Analgesics Physiotherapy - active Radiculopathy Surgical Indications Intractable radicular (not axial) pain which has failed conservative management Progressive or significant neurological deficit Spine Pain – Red Flags Hx of major trauma or minor trauma in elderly, osteoporotic patients Age < 20 or > 50 Hx of cancer, fever, chills, unexplained wt. loss Hx of recent infection, IV drug abuse, immunocompromise Hx of bladder or bowel incontinence, urinary retention Hx of major or progressive neurological deficit Hx of pain worsening when supine or severe night pain Spine Pain – Red Flags Exam: major neurological deficit/signs of upper motor neuron dysfunction Exam: peri-anal anaesthesia Exam: loss of anal sphincter tone Indications for Surgery (Non-Degenerative Back Pain) Tumour – primary – metastatic Infection – Discitis/osteomyelitis – Epidural Abcess Fracture/subluxation with instability Clinical Assessment of Spinal Injuries History Mechanism of injury Spinal pain Paraesthesia or motor weakness Physical examination Log roll, inspect and palpate entire spine Tenderness Malalignment of spinous processes Traps for the Unwary Patient intoxication Altered level of consciousness Distraction from other injuries Cursory examination – failure to appreciate single root injury Cervical Spine X-rays Lateral to T1 AP Open-mouth odontoid CT Scan if one or more of above not available Treatment of Spine Injuries Immobilize patient Reduce deformity Stabilize/fuse spine Back to Basics for Surgery Peripheral Nerve Injury Classification (Seddon) • Neurapraxia • Axonotmesis • Neurotmesis Peripheral Nerve Injury History – Usually immediate onset of symptoms/signs from time of injury – Blunt or penetrating injury – Blunt injury frequently associated with fracture or dislocation – May follow reduction of fracture or dislocation – Delayed onset: compartment syndrome or vascular injury to limb Peripheral Nerve Injury Physical Examination – – – – Upper vs. lower motor neuron Root vs. peripheral nerve Which root? Which peripheral nerve? Investigations MRI/CT – Indirect, helpful if question of upper vs. lower motor neuron, root vs. peripheral nerve EMGs/Nerve conduction – Former useful, latter not – Most sensitive in detecting early recovery – Not useful in acute management Extremity X-rays: – helpful with injury site if fracture or dislocation Investigation • EMG (all injuries) importance of clinical vs. EMG recovery • Root and trunk injuries Metrizamide CT- myelogram MRI Overall Treatment Strategy • Nerve repair Restore movement Restore sensation • Muscle/tendon/joint reconstructive surgery • Prosthetics • Rehabilitation • Educational and vocational advice Timing of Surgery • Primary repair (penetrating injury) immediate delayed (2 weeks) • Secondary repair (blunt injury) 3 - 4 month delay Reconstructive Strategies to Achieve Elbow Flexion • Steindler flexoroplasty • Latissimus dorsi transfer • Pectoralis major transfer • Triceps transfer Common Wrist/Hand Tendon Transfers • Wrist extension -- pronator teres • Thumb extension -- palmaris longus • MCP extension -- flexor carpi radialis • Finger flexion -- brachioradialis or extensor carpi radialis longus to flexor digitorum profundus • Thumb flexion -- BR or ECRL to FPL Results Etiology Etiology No. of Pts Lacerations MVA Winter sports Falls Gunshot wounds Others 24 22 11 8 4 14 Adjacent fractures in 15 patients Individual nerve outcome Nerve Inc. loss to f/u Brachial plexus 33% Axillary 42.9% Musculocutaneous 57.1% Radial 58.3% Median 75% Ulnar 66% Posterior tibial 50% Exc. loss to f/u 37.5% 75% 80% 87.5% 85.7% 100% 60% Outcome by Etiology Laceration MVA Winter sports Falls 87.5% 32% 57.1% 50%