Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Epidemiology wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Public health genomics wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Alzheimer's disease research wikipedia , lookup
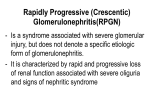
Glomerulonephropathy Internal Medicine Lecture Series September 20, 2006 Dolan Wenner D.O. Glomerulonephritis Inflammation of the glomeruli of the kidney Inflammation causes a decrease in the kidney’s ability to filter substances out of the bloodstream Blood Protein Lipids Glomerulonephritis Inflammation causes damage to the major components of the glomerulus Epithelium Basement Membrane Capillary Endothelium Mesangium Glomerulus Glomerulus (EM) Major Determinants of Glomerular Injury The nature of the primary insult and secondary mediator systems it invokes The site of injury within the glomerulus The speed of onset, the extent, and intensity of disease Primary vs. Secondary Primary Glomerular Disease Disorders in which the glomerulus is the sole or predominant tissue involved. These diseases are typically idiopathic. Secondary Glomerular Disease Glomerular injury is a feature of a systemic disease involving multiple organs or systems. Primary Insult Immunologic Metabolic Hemodynamic Toxic Deposition Infectious Inherited Acute, Subacute, & Chronic Acute injury occurring over days to weeks Subacute injury rapidly progressive over weeks or months Chronic injury occurring over months to years Focal vs. Diffuse Focal lesions involve less than 50% of the glomerulus Diffuse lesions involve greater than 50% of the glomerulus Segmental vs. Global Segmental lesions involve only part of the glomerular tuft Global lesions involve almost all of the glomerular tuft Intracapillary vs. Extracapillary Intracapillary refers to endothelial or mesangial cells Extracapillary refers to Bowman’s space Classification of Glomerulopathy Nephritic syndrome Nephrotic syndrome Nephritic Syndrome Presents with sudden onset of hematuria (RBC casts hallmark) and variable proteinuria (<3g/24 hrs) Decreased GFR with increase in BUN and creatinine Nephritic Syndrome Signs and symptoms Oliguria Macroscopic hematuria (smoky-brown urine) Hypertension Possibly edema in low-pressure areas (periorbital and scrotal areas) Nephritic Syndrome Causes Post-streptococcal glomerulonephritis IgA nephropathy (Berger’s disease) Wegener’s granulomatosis Alport’s syndrome Goodpasture’s syndrome SLE Post-streptococcal Glomerulonephritis Group A β-hemolytic strep H & P Oliguria, edema, htn., smokybrown urine Labs and Histology Low serum C3, increased ASO titer, lumpy-bumpy immunofluorescence (IF) Treatment supportive, most have complete recovery Post-Streptococcal Glomerulonephritis IgA Nephropathy (Berger’s disease) Most common type of nephritic syndrome, associated with upper respiratory or GI infections; commonly in young men H & P gross hematuria Labs and Histology may see elevated serum IgA; biopsy and IF will show mesangial IgA deposits Treatment corticosteroids; 20% progress to ESRD IgA Nephropathy Wegener’s Granulomatosis Granulomatous inflammation of the respiratory tract and kidney with necrotizing vasculitis H & P fever, wt. loss, hematuria, respiratory and sinus symptoms; cavitary pulmonary lesions bleed and cause hemoptysis Labs and Histology c-Anca (cell mediated immune response) Treatment High-dose corticosteroids and cytotoxic agents; pts tend to have frequent relapses Alport’s syndrome Hereditary glomerulonephritis; present in boys 520 years old H & P asymptomatic hematuria associated with nerve deafness and eye disorders Labs and Histology GBM splitting on electron microscopy Treatment Progresses to renal failure; antiGBM nephritis may recur after transplant Alport’s syndrome Goodpasture’s syndrome Glomerulonephritis with pulmonary hemorrhage; peak incidence in men in their mid-20s; an immune form of RPGN H & P hemoptysis, dyspnea, possibly respiratory failure Labs and Histology linear anti-GBM on IF, iron deficiency anemia, hemosiderin-filled macrophages in sputum, pulmonary infiltrates on CXR Treatment plasma exchange therapy, pulsed steroids; may progress to ESRD Goodpasture’s Syndrome Nephritic Syndrome Treatment Treat hypertension, fluid overload, and uremia Salt and water restriction Diuretics Dialysis if necessary Protein restricted to approx. 1 g/kg/day Corticosteroids are sometimes useful to decrease glomerular inflammation Treat underlying disease; possible biopsy for diagnosis Nephrotic Syndrome Defined as > 3.5 g urinary protein/24 hrs, albumin < 3 g/dL, and peripheral edema. Pts. may also have associated hyperlipidemia and hypercoagulable states Nephrotic Syndrome Causes Minimal change disease Focal segmental glomerulosclerosis Membranous nephropathy Diabetic nephropathy Lupus nephropathy Renal amyloidosis Membranoproliferative nephropathy Minimal Change Disease Idiopathic etiology; common in children H & P tendency toward infections and thrombotic events Labs and Histology light microscopy appears normal; electron microscopy shows fusion of epithelial foot processes with lipid-laden renal cortices Treatment steroids; excellent prognosis Minimal Change Disease Focal Segmental Glomerulosclerosis (FSGS) Idiopathic, IVDU, HIV infection H & P typical patient is young black male with uncontrolled htn. Labs and Histology microscopic hematuria; biopsy shows sclerosis in capillary tufts Treatment prednisone, cytotoxic therapy Focal Segmental Glomerulosclerosis Membranous Nephropathy Most common Caucasian adult nephropathy; an immune complex disease H & P associated with HBV, syphilis, malaria, and gold Labs and Histology “spike and dome” appearance due to granular deposits of IgG and C3 at basement membrane Treatment prednisone and cytotoxic therapy for severe disease Membranous Nephropathy Diabetic Nephropathy Two characteristic forms: diffuse hyalinization and nodular glomerulosclerosis (KimmelstielWilson lesions) H & P long standing, poorly controlled DM Labs and Histology thickened GBM; increased mesangial matrix Treatment tight control of blood sugar; protein restriction; ACEIs Diabetic Nephropathy Lupus Nephritis Both nephrotic and nephritic; severity determines prognosis H & P proteinuria or RBCs on UA may be found in SLE pts Labs and Histology mesangial proliferation; subendothelial immune complex deposition Treatment prednisone and cytotoxic therapy may slow disease progression Lupus Nephritis Renal Amyloidosis Primary (plasma cell dyscrasia) and Secondary (infectious or inflammatory) most common H & P may have multiple myeloma or a chronic inflammatory disease (e.g. rheumatoid arthritis, TB) Labs and Histology abdominal fat biopsy; seen with Congo red stain; apple-green birefringence under polarized light Treatment prednisone and melphalan; bone marrow transplant may be used for multiple myeloma Renal amyloidosis Membranoproliferative nephropathy Can also be a nephritic syndrome H & P slowly progressing renal failure Labs and Histology “Tram-track” double layered basement membrane; Type I has subendothelial deposits, Type II involves a C3 nephritic factor and decreased C3 Treatment corticosteroids and cytotoxic agents may help Membranoproliferative Nephropathy Nephrotic Syndrome Treatment Treat proteinuria Low salt and saturated fat diet Limited protein intake Furosemide for peripheral edema If diabetic consider ACEi Fluid restriction (hyponatremia) Statin for hyperlipidemia Anticoagulation for pts. with thrombosis May need biopsy for diagnosis Clinical Manifestations of Glomerular Disease Asymptomatic proteinuria Nephrotic syndrome (proteinuria, hypoproteinemia, hyperlipidemia, edema) Asymptomatic hematuria Glomerulonephritis (hematuria, proteinuria, hypertension, renal failure) Clinical Manifestations of Glomerular Disease (con’t) Acute glomerulonephritis (nephritis with short term renal failure) Crescentic Glomerulonephritis (nephritis with rapidly progressive renal failure) Chronic Glomerulonephritis (chronic progression of renal failure) End Stage Renal Disease (irreversible renal failure) Question 1 Which of the glomerulopathies shows a characteristic “tram-track” double layered basement membrane? a. Minimal change disease b. Membranoproliferative nephropathy c. Focal Segmental Glomerulosclerosis d. Berger’s Disease Question 1 Which of the glomerulopathies shows a characteristic “tram-track” double layered basement membrane? a. Minimal change disease b. Membranoproliferative nephropathy c. Focal Segmental Glomerulosclerosis d. Berger’s Disease Question 2 Which of the following is present in Wegener’s granulomatosis? a. p-Anca b. d-Anca c. c-Anca d. s-Anca Question 2 Which of the following is present in Wegener’s granulomatosis? a. p-Anca b. d-Anca c. c-Anca d. s-Anca Question 3 Which class of medications is indicated in patients with diabetic nephropathy? a. ACEIs b. NSAIDs c. Macrolides d. Aminoglycosides Question 3 Which class of medications is indicated in patients with diabetic nephropathy? a. ACEIs b. NSAIDs c. Macrolides d. Aminoglycosides Thank You!