Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
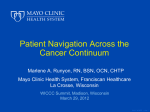
Cerebellopontine Angle Cavernous Angioma: In the Setting of Multiple Familial Cavernous Malformations Justin Mauch, M.D.; Carrie Carr, M.D.; Norbert Campeau, M.D. Mayo Clinic, Rochester MN Department of Radiology ASNR 53rd Annual Meeting April 25 - 30th, 2015 Chicago, Illinois, USA Control #: 542 Poster #: EE-05 April 27th, 2015 ©2015 MFMER | slide-1 Disclosures • None ©2015 MFMER | slide-2 Purpose • To present a case of cerebellopontine angle (CPA) cavernous malformation occurring in the setting of Multiple Familial Cavernous Malformations. • The distinguishing imaging and clinical features of this rare lesion, which was initially diagnosed as a vestibular Schwannoma, will be highlighted. ©2015 MFMER | slide-3 Case Report • 58 year old male presented with multiple insidiously progressive neurologic deficits • • • • Neurogenic bladder Poor right leg motor and balance function Dizziness Right-sided hearing loss • Initial work-up: • Neurologic evaluation • MRI brain and MRI cervical/thoracic spine • Audiometry ©2015 MFMER | slide-4 Imaging Findings: Initial MRI A B C D C E F Selected axial T2WI of the brain (A-D) and T1 pre and post gadolinium (E and F respectively) demonstrate multiple intracranial and spinal cord (not shown) lesions with findings characteristic of cavernous malformations leading to the diagnosis of Multiple Familial Cavernous Malformations. ©2015 MFMER | slide-5 Imaging Findings: CT B C A A head CT was never performed, however a CT myelogram was obtained for evaluation of cervical myelopathy related to cervical spinal cord cavernous malformations. The CT (A) demonstrated a noncalcified mass in the right CPA (arrow). A spinal cord mass at C5-6 is shown on the sagittal CT Myelogram (B) with MR imaging characteristics of a cavernous malformations as seen on sagittal T2WI (C). ©2015 MFMER | slide-6 Case Report • A right CPA mass was identified • It demonstrated homogenous enhancement and partial extension into right IAC • Findings were suggestive of an incidental vestibular schwannoma. ©2015 MFMER | slide-7 Imaging Findings: Initial MRI A The MRI demonstrates a right CPA mass (arrows) with areas of T2 (A) hyperintensity and homogenous enhancement as seen on pre-contrast T1 (B) and post-contrast T1 (C). B C *All sections at same level ©2015 MFMER | slide-8 Case Report • Patient had vestibular and audiometric testing: • Decreased right sided function • Patient elected to forego surgical intervention or gamma knife therapy due to the stability of his deficit. ©2015 MFMER | slide-9 Case Report • Follow-up imaging was performed over the next decade • Most recently due to hemorrhagic complication of multiple intracranial and spinal cord cavernous malformations with eventual resection • Follow-up MR imaging included high resolution FIESTA and susceptibility weighted sequences ©2015 MFMER | slide-10 Imaging Findings: 10 year Follow-Up MRI imaging 2004 2014 Axial T1 post gadolinium images from the MRI follow-up over the next decade demonstrated subtle changes in the CPA lesion size and appearance, with most apparent change noted on the 2014 MRI, where the lesion enlarged and become more heterogenous in appearance. ©2015 MFMER | slide-11 Imaging Findings: CPA lesion changes appearance The 2014 follow-up MR imaging included pre-contrast T1 (A), high resolution FIESTA (B), post-contrast T1 (C), and susceptibility weighted sequences (D). A B C D New T1 (A) hyperintense signal changes within the right CPA lesion with associated low signal on SWI (D), compatible with subacute blood products. FIESTA imaging (B) also better demonstrates that the mass does not extend into the IAC, not the typical configuration for a Schwannoma The CPA lesion now has findings consistent with a cavernous malformation rather than Schwannoma. ©2015 MFMER | slide-12 Discussion • Cavernous malformations of the CPA are rare entities which make up an estimated 0.0023% of all CPA lesions* • To date, there are only two other reported cases of a CPA cavernous malformation occurring in the setting of Multiple Familial Cavernous Malformations (Aquilina, Cotton) • Surgical options for CPA Schwannoma or Meningioma include primary microsurgery, stereotactic radiosurgery, or observation* • It is important to differentiate a CPA cavernous malformation from these more common CPA lesions due to surgical planning. CPA cavernous malformation are highly vascular and can present with copious intraoperative hemorrhage* • Microsurgical gross total resection has been proposed as the treatment of choice as subtotal resection can result in *Kohan, Carlson, Park, Barrera, Deshmukh, Safronova recurrence* ©2015 MFMER | slide-13 Discussion Distinguishing Imaging Features… • Specific imaging features of CPA cavernous malformation can help to distinguish it from other more common CPA lesions, such as Schwannomas and Meningiomas • Schwannomas and Meningiomas both enhance strongly after gadolinium injection while cavernous malformations will have mild heterogeneous enhancement* • Hyperintense T1 signal and susceptibility artifact suggest blood product which is typically not seen with Meningiomas or Schwannomas* • Schwannomas are often T2 hyperintense while cavernous malformations will have areas of low T2 signal • Schwannomas will typically have a component within the IAC • CT may show areas of calcification within CPA cavernous malformations where as this is less common in Schwannomas *Bonneville ©2015 MFMER | slide-14 Imaging Differential Diagnosis Below: Right CPA Schwannoma. Axial T1 (A), Axial FIESTA (B), and Axial T1+ Gd (C). A B C Below: Right CPA Meningioma. Axial T1 (A), Axial FIESTA (B), and Axial T1+ Gd (C). A B C Below: Right CPA cavernous malformation. Axial T1 (A), Axial FIESTA (B), and Axial T1+ Gd (C). A B C ©2015 MFMER | slide-15 Imaging Findings: Use of Susceptibility Weighted Imaging SWI (A) and Axial T2 FSE and (B) images obtained at the same level illustrates the utility of detecting hemosiderin with the SWI technique. SWI images (C) and Axial T2 FSE (D) obtained at the level of the CPA lesion. The SWI confirms presence of hemosiderin within the right CPA cavernous malformation (arrows). A B C D ©2015 MFMER | slide-16 Summary • Cavernous malformations of the CPA are rare entities, but consideration of this diagnosis is important when specific imaging and clinical features are present. • Hyperintense T1 signal within the lesion and blooming on susceptibility weighted imaging indicative of old blood products are suggestive of this lesion, and essentially diagnostic in individuals with Multiple Familial Cavernous Malformations. • Accurate preoperative diagnosis is important for planning appropriate surgical removal of this highly vascular mass. ©2015 MFMER | slide-17 References • Adachi K, Yoshida K, Akiyama T, et al. Cavernous angioma of the vestibular nerve: case report and literature review. Surg Neurol 2008; 70:82-86. • Carlson ML1, Tveiten OV, Driscoll CL, Goplen FK, Neff BA, Pollock BE, Tombers NM, Castner ML, Finnkirk MK, Myrseth E, Pedersen PH, Lund-Johansen M, Link MJ. Long-term quality of life in patients with vestibular schwannoma: an international multicenter cross-sectional study comparing microsurgery, stereotactic radiosurgery, observation, and nontumor controls. J Neurosurg. 2015 Jan 2:1-10. • Park SH1, Kano H, Niranjan A, Flickinger JC, Lunsford LD. Stereotactic radiosurgery for cerebellopontine angle meningiomas. J Neurosurg. 2014 Mar;120(3):708-15. • Cotton CA, Beall DP, Winter BJ, et al. Cavernous angioma of the cerebellopontine angle. Curr Probl Diagn Radiol 2006; 35:120-123. • Safronova MM, Vaz AR, Resende M, et al. Cavernous malformation of the internal auditory canal: a diagnostic challenge. Otol Neurotol 2009;30:1015Y7 • Barrera JE, Jenkins H, Said S. Cavernous hemangioma of the internal auditory canal: a case report and review of the literature. Am J Otolaryngol 2004;25:199-203. • Deshmukh VR, Albuquerque FC, Zabramski JM, Spetzler RF. Surgical management of cavernous malformations involving the cranial nerves. Neurosurgery 2003;53:352-7. • Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontine angle lesions: an update. Part 1. Enhancing extra-axial lesions. Eur Radiol 2007; 17:2472– 2482 • Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontinenangle lesions: an update. Part 2. Intra-axial lesions, skull base lesions that may invade the CPA region, and non-enhancing extra-axial lesions. Eur Radiol 2007; 17:2908–2920 • Kohan D, Downey LL, Lim J, Cohen NL, Elowitz E. Uncommon lesions presenting as tumors of the internal auditory canal and cerebellopontine angle. Am J Otol. 1997;18:386–92 • Aquilina K1, Nanra JS, Brett F, Walsh RM, Rawluk D. Cavernous angioma of the internal auditory canal. J Laryngol Otol. 2004 May;118(5):368-71. • Samii M, Nakamura M, Mirzai S, Vorkapic P, and Cervio A. Cavernous angiomas within the internal auditory canal. J Neurosurg 2006; 105:581-587 ©2015 MFMER | slide-18