Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
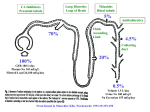
Chronic Heart Failure When Should You be Worried? James C. Fang, MD Heart Failure, Transplantation, and Circulatory Assistance Program University Hospitals/Case Medical Center Heart Failure Progressive, incurable, and ultimately fatal • Stage A At high risk for HF but no structural heart disease • Stage B Structural heart disease but w/o signs or symptoms of HF • Stage C Structural heart disease with prior or current symptoms • Stage D Refractory HF requiring specialized interventions Hunt et al., Circulation 2001;104:2996 • HTN, DM, CAD, cardiotoxins • LVH, LVSD, MI, asx valve dz • Sx LVSD or asx on Tx • Recurrent hosp, need for Tx/VAD Heart Failure is Increasing Baker, WH et al. Circulation, Feb 2006; 113: 799 - 805 And Heart Failure Mortality Remains High Levy D et al. N Engl J Med 2002;347:1397-1402 Mortality in End-Stage Heart Failure One-year survival rates AIDS: 90% Leukemia: 64% Lung cancer: 42% Pancreatic cancer: 21% End-stage heart failure with optimum medical management: 25% • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec HF hospitalization is ominous Risk of death increases three-fold after HF hospitalization Solomon SD, et al. Circulation 2007;116:1482-1487 • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec CRT Nonresponders So What? For CRT nonresponders, Consider 1) 2) 3) 4) 5) It’s common (25-33%) Definition of NR Lead review or revision Reprogramming Advanced HF referral Cha, Yong-Mei, et al. J Cardiovasc Electrophysiol 2007;18:1015-1019 • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec ACE Inhibitor Intolerance: Marker of Severe Disease ACEI No ACEI • 259 consecutive HF Age 55 60 admissions to BWH If they can’t tolerate RAS antagonists, CAD 43% 65% • 23% not on ACEI at d/c due Duration 2 5 Be very worried to circulatory-renal NYHA 3-4 50% 82% limitations: Creatinine 1.2 2.5 – symptomatic BP – renal insufficiency Death* 22% 57% – hyperkalemia *median follow-up, 8.5 months Pinto et al., JACC 2003 • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec If you hear a third heart sound in the office… SOLVD treatment Trial • 2569 pts w/ CHF • Enalapril vs placebo • Baseline examinations • Death or Hospitalization for CHF • RR 1.30 (1.11-1.53, p<0.005) • Adjusted for EF, NYHA, BP, HR, Na, Cr, Age Drazner MH, NEJM 2001;345:574 • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec Escalating Creatinine in Heart Failure Populations 2 1.9 1.8 1.7 1.6 1.5 1.4 1.3 1.2 1.1 1 SOLVD CONSENSUS RALES COPERNICUS ESCAPE REMATCH SOLVD: Impact of Renal Insufficiency * Total Mortality, % 50 40 *p<0.001 30 20 * 10 0 SOLVD Prevention CrCl > 60 SOLVD Treatment CrCl < 60 Dries et al., J Am Coll Cardiol 2001 Mortality Risk of Decompensated Heart Failure 1) BUN > 43 mg/dL 2) SBP <115 mmHg 1) BUN > 43 mg/dL 2) SBP <115 mmHg 3) SCr > 2.75 mg/dL 3) SCr > 2.75 mg/dL Fonorow G, et al. JAMA 2005 Decompensated Heart Failure CART analysis Azotemia confers a high mortality Fonorow G, et al. JAMA 2005 Prognostic Significance of Worsening Renal Function During HF Admission *Worsening Renal Function = Cre 0.3 No WRF (n=731) WRF (n=273) LOS > 10 days 9% 28% Complication 20% 38% Mortality 1% 7% Gottlieb et al., J Card Failure 2002:8;136 When the Creatinine Rises… • • • • • • • • • Patient can’t go home Diuretic doses are often decreased ACE inhibitors/ARBs are often discontinued Other medications are renally dosed Inotropes may be initiated PA catheter may be placed Foley catheter may be re-placed Cardiac US may be ordered Renal US may be ordered (and is rarely helpful) Worsening Renal Function and CHF Who’s at risk? Hazard Ratio Weight H/o CHF 1.3 1 DM 1.4 SBP>160 % WRF RR 0 9.8 1.0 1 1 18.7 1.9 1.4 1 2 20.3 2.1 1.5 ≤ Cr ≤ 2.5 2.1 2 3 30.3 3.1 Cr ≥ 2.5 3.5 3 4+ 52.8 5.4 Risk Factor Forman, JACC 04 Score P<0.001 Diuretics Decrease GFR in HF 15 10 GFR (% change) N = 16 NYHA III LVEF = 28% Placebo 5 0 -5 80 mg IV Furosemide -10 -15 -20 -25 0 500 1000 1500 2000 2500 Cumulative Urine Output, 0–8 h (mL) Gottlieb et al., Circulation 2002;105:1348 Hemodynamic Response to IV Furosemide in Heart Failure Hemodynamic Baseline 20 min after Lasix 40 mg IV P PAWP (mm Hg) 28 ± 7 33 ± 9 <0.01 SVI (mL/min/m2) 27 ± 8 24 ± 7 <0.01 HR (bpm) 87 ± 13 91 ± 16 <0.01 MAP (mm Hg) 90 ± 15 96 ± 15 <0.01 SVR (dyne • s/cm5) 1454 ± 394 1676 ± 415 <0.01 PRA (ng/mL) 9.9 ± 8.5 17.8 ± 16 <0.05 PNE (pg/mL) 667 ± 390 839 ± 368 <0.01 Francis et al., Ann Int Med 1985;103:1 Diuretics and arrhythmic death? Cooper HA, et al. Circulation 1999;100:1311-1315 Diuretic Resistance “a clinical state in which diuretic response is diminished or lost before the therapeutic goal of relief from edema has been reached” “Braking Phenomenon” A decrease in response to a diuretic after the first dose Mechanisms 1) 2) 3) 4) 5) Poor oral bioavailability Tubular hypertrophy to compensate for salt loss Renal insufficiency Neurohormonal mechanisms Reduced renal blood flow Brater DC. N Engl J Med. 1998;339:387 When the Diuretics Don’t Work…. • • • • • Restrict daily fluid intake (1.0-1.5 L) Aggressive restriction of daily salt intake (≤2 g) Stop NSAIDs Decrease beta blockade Give PO short-acting loop diuretic in several divided (and increasing) doses, bolus, or continuous IV administration • ?Nesiritide • Use sequential nephron blockade by adding to loop diuretic – thiazide diuretic – Aldosterone antagonist – short-term acetazolamide More than 50% of Patients Have Little or no Weight Loss During Hospitalization 33% 35 Patients (%) 30 24% 25 20 13% 15 10 7% 15% 6% 5 3% 2% (5 to 10) (>10) 0 (<-20) (-20 to -15) (-15 to -10) (-10 to -5) (-5 to 0) (0 to 5) Change in Weight (lbs) Fonarow GC. Rev Cardiovasc Med. 2003; 4 (Suppl. 7): 21 Inotropic Therapy: Variable Effects Colucci et al., Circulation 1986;73:III175 Mortality in Large Placebo-Controlled Trials of Inotropes for Heart Failure Trial Inotrope NYHA N Mortality vs Placebo VEST Vesnarinone III, IV 3833 11% Increase Xamoterol Xamoterol III, IV 516 Hazard ratio: 2.5 PRIME II Ibopamine III, IV 1906 Hazard ratio: 1.26 PICO Pimodendan II, III 317 Hazard ratio: 1.8 Inotropes should not be used for the PROMISE Milrinone III, IV 1088 28% Increase routine management of the cardiorenal syndrome PROMISE = Prospective Randomized Milrinone Survival Evaluation; VEST = Vesnarinone Trial; PRIME = Prospective Randomized Ibopamine Mortality Evaluation; PICO = Pimobendan in Congestive Heart Failure Felker GM, O’Connor CM. Am Heart J. 2001;142:393–401. Hemodynamics and Aggravated Renal Dysfunction No ARD + ARD RAP 12 9 12 10 Cardiac index 2.1 2.4 2.3 2.3 SVR 1470 1100 1400 1200 Renal Perf Press 67 66 61 64 No obvious hemodynamic difference….. Weinfeld, Chertow, Stevenson Am Heart J 1999 Neurohormonal Regulation of Renal Function in CHF SNS RAAS Endothelin Arginine Vasopressin Adenosine Natriuretic Peptides Prostaglandins Nitric Oxide Bradykinin Vasocontrictors Na/H20 Retentive Vasodilators Na/H20 Excretory Decompensated HF No Standard of Care • Wide variability in clinical practice • Few randomized controlled trials • Guidelines focus on: – stable outpatients – systolic (“low EF”) HF • Intravenous versus oral agents • Unclear endpoints to hospitalization • What is appropriate post-discharge care? What are the options? • • • • • • Hemodynamic guided management Vasopression antagonists (“Vaptans”) Adenosine antagonists Natriuretic peptides Ultrafiltration Advanced HF referral Ultrafiltration for Fluid Retention in Heart Failure • • • • • • Acute reductions in filling pressures CO - no change or increased Serum norepinephrine levels decreased Improved lung compliance Improved exercise capacity Mixed effects on renal function Guazzi et al 1987,1990 Fauchald et al, 1986 Simpson et al,1985 Agostini et al,1993 Inoue et al, 1992 UF in refractory CHF • 24 pts with Class IV HF – >5 kg weight gain – oliguria • Single UF session in CCU – mean time 9 hours – mean volume removed 4,880 ml • Results – No hypotension – Increased CO – Decrease SVR Marenzi JACC 2001 Ultrafiltration in Diuretic Resistance Decreasing Length of Stay EUPHORIA Trial 19 pts w/ CHF and diuretic resistant • Furosemide > 80 mg • SCr > 1.5 mg/dl • Before IV diuretics Avg 8367 4232 cc removed 2.6 treatments No readm w/in 30d CHF Solutions • • • • • • • • • Ultrafiltration, not dialysis Two Peripheral IVs (CL preferred) 100-500 ml/hr fluid removal over 24 hrs Extracorporeal blood volume ~ 40 ml Little hemodynamic effect Systemic anticoagulation suggested Limited need for nursing support Minimal electrolyte shifts (isotonic filtrate) Greater total body Na removal than diuretics for given volume The UNLOAD Trial Efficacy • Weight loss at 48 hours after randomization • Dyspnea score at 48 hours after randomization Safety • Changes in serum blood urea nitrogen, creatinine, and electrolytes at 8, 24, 48 and 72 hours after randomization, discharge, 10, 30 and 90 days • Episodes of hypotension during the first 48 hours after randomization The UNLOAD Trial • Ultrafiltration arm • Ultrafiltration rate ≤ 500 cc/hour • Duration/rate of fluid removal decided by treating physicians • IV diuretics prohibited during ultrafiltration • Standard Care arm • IV diuretics as bolus or continuous infusions • IV doses ≥ 2 times daily PO dose for the first 48 hours after randomization Primary PrimaryEnd End Point Point Weight Weight Loss Loss at at 48 48 Hr Hr Freedom From Re-hospitalization for Heart Failure UF decreased: 1) % pts requiring re-hospitalization 2) Number of HF re-hospitalizations 3) Days of re-hospitalization for HF 4) ED and unscheduled office visits Safety End Points: Change in Serum Creatinine • 53 year old man admitted with weight gain and dyspnea despite increasing loop diuretics – – – – Third admission this year Idiopathic CMP (EF 25%) PAF w/ inappropriate ICD shocks CRT 6 months prior • Meds: carvedilol, digoxin, torsemide, aldactone, coumadin – No ACEI/ARB because of worsening renal function • BP 100/80, HR 85, R 22, JVD to jaw, clear lungs, S3, TR, MR, loud P2, palp liver edge, distended abd, no edema • Hct 30%, Na 130, BUN 55, Cr 2.5, EKG afib, QRS 130 msec When to get worried… • • • • • Recurrent hospitalizations CRT nonresponders Persistence of thirdget heart sound with on exam (It won’t better time) Inability to tolerate RAS antagonists and/or beta blockers Renal insufficiency is present • • • • • Poor or worsening functional capacity RV dysfunction is present High BNP levels Recurrent ventricular arrhythmias “Diastolic HF” in absence of hypertension Medically Refractory Heart Failure? • Persistent symptoms despite: – – – – RAS antagonism with ACEI/ARB/Aldo antagonists Beta blockers titrated to target doses Device therapy (ie. ICD/CRT) Addressing comorbidities (e.g. sleep apnea, anemia, etc.) – Participation in HF Disease Management Program • Inability to establish euvolemia without aggravating renal function • Inability to keep out of the hospital