Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
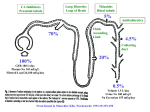
Resistencia de Diuretico….ó Resistencia del Doctor y el Paciente? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Albert Einstein College of Medicine Associate Chief for Academic Affairs – Cardiology Head Clinical Trials, Cardiology Montefiore-Einstein Medical Center Bronx, NY Outcomes During and After ADHF In-hospital1 – Length of stay (mean) 6.2 days – Mortality rate 4.1% Hospital readmissions2 – 20% at 30 days – 60-90 days • 24% in Euro-HF • 30% in OPTIMIZE-HF – 50% at 6 months Longer-term mortality3 – 11.6% at 30 days – 33.1% at 12 months 1. Fonarow GC, et al. JAMA. 2005;293:572-580. 2. Gheorghiade M, et al. Circulation. 2005;112:3958-3968. 3. Jong P, et al. Arch Intern Med. 2002;162:1689-1694. 2 Important Comorbidities in ADHF ● ● ● ● ● ● ● ● ● Hypertension Coronary artery disease Myocardial infarction Stroke/transient ischemia attack Atrial fibrillation Chronic renal insufficiency Hyponatremia Diabetes COPD/asthma Teerlink JR. Diagnosis and Management of Acute Heart Failure. In: Libby P, Bonow RO, Mann DL, Zipes DP, eds. Braunwald’s Heart Disease. 8th ed. Philadelphia PA: Saunders Elsevier; 2008:583-610. 3 Diuretics in AHF Mechanism of action – Diuresis (decreased preload) – ? Pulmonary vasodilation Advantages – Rapid symptomatic improvement – Decreases volume overload Disadvantages – – – – Increased neurohormonal activation Electrolyte disturbances, arrhythmias Worsen renal function High diuretic doses associated with increased hospitalization and mortality Hunt SA, et al. Circulation. 2009;119:e391-e479. 4 Mechanisms of Sodium and Water Retention in Heart Failure Chronic Decrease in Cardiac Output Or Decrease in Peripheral Vascular Resistance Increased Cardiac Filling Pressures Absolute or Relative Decrease in Arterial Blood Volume Water Retention V2 Receptors Stimulation Baroreceptor Desensitization Decreased Renal Perfusion Pressure Renal Vasoconstriction Nonosmotic AVP Release Increased Sodium and Water Retention Resistance to Natriuretic Peptides Failure to Escape From Aldosterone Increased SNS Activity Increased RAAS Activity Decreased GFR Increased Water and Sodium Reabsorption in the Proximal Tubule Reduced Distal Delivery of Sodium Adapted from Schrier RW: J Am Coll Cardiol 2006; 47:1-8 Sodium Reabsorption and Diuretics Sites of Action in the Nephron Diuretics: Beneficial Effects Congestive Heart Failure Loop Diuretics or Ultrafiltration Negative Sodium and Water Balance Decreased Functional Mitral Insufficiency Decreased Ventricular Dysfunction Improved Myocardial Function Improved Renal Function Improved Pulmonary Congestion Decreased Cardiac Filling Pressures Decreased Ventricular Wall Stress and Endomyocardial Ischemia Pharmacokinetics of Loop Diuretics Loop Diuretic Oral Bioavailability (%) Why is this important in HF? 1. Hepatic Congestion 2. Gut Edema 3. ↓ Gut Blood Flow Elimination Half-Life (hr) Norm al Subje cts Patients with Renal Insufficiency Patients with Heart Failure Furosemide 10-100 1.5-2 2.8 2.7 Bumetanide 80-100 1 1.6 1.3 Torsemide 80-100 3-4 4-5 6 Causes of Diuretic Resistance Inadequate Dose Patient Non Compliance – Not taking drug – High NaCl Intake Poor Absorption Impaired Secretion – Chronic Kidney Disease – Old Age – Kidney Transplant – Chronic Heart Failure – Drugs • NSAIDs • Probenecid Proteinuria Hypoproteinemia Hypotension Drugs-Direct Inhibitors – NSAIDs Diuretic Tolerance (Structural/Functional Adaptation) glomerular hypertrophy Neurohormonal Activation ‘Cardiorenal Limit’ Inadequate Dosing AM PM + FENa Log Diuretic Concentration Ineffective Effective Dose Dose =0 FENa Log Diuretic Concentration Ineffective Effective Dose Dose Ellison DH. Cardiology 2001; 96:132–143 Sodium Intake Influences Diuretic Effect! Diuretic Secretion Is Impaired in CKD Uremic anions block diuretic secretion into the proximal tubule Diuretics Act from the tubule lumen D Uremic Loop Diuretics Na K Cl Anions + K Na D Diuretic Albumin Ellison DH. Cardiology 2001; 96:132–143 D D Dose-Response Curves for Loop Diuretics Ellison DH. Cardiology 2001; 96:132–143 PREVALENCE AND SEVERITY OF RENAL DYSFUNCTION IN PATIENTS ADMITTED WITH ADHF 45.7 50 Males 41.2 45 Females Prevalence (%) 40 30 35 24.9 30 25 20 15 14.6 11.5 10.6 6.6 7.3 7.5 10 5 0 I II III IV V Kidney Function Stage Heywood JT, Fonarow GC, Costanzo MR et al. J Cardiac Fail 2007;13:422-30 Loop Diuretics Stimulate Renin + Na K Cl Renin - MD K Na LOOP DIURETIC + Na K Cl - K TAL Na Ellison DH. Cardiology 2001; 96:132–143 Neurohormonal Actions Influencing Diuretic Action Glomerulus Norepinephrine, Endothelin, AII decrease renal blood flow and GFR Proximal Tubule AII Increases Na Reabsorption Collecting Duct Aldosterone Increases Na Reabsorption Impact of Worsening Renal Function on Heart Failure Outcomesa Outcome RF not worse RF worse OR (95% CI) In-hospital mortality 3% 7% 2.7 (1.6-4.6) 30-day mortality 6% 10% 1.9 (1.3-2.8) 6-month mortality 19% 25% 1.6 (1.2-2.1) Length of stay, d 6.93 9.14 2.28 (0.25)b a1681 patients age ≥65 years, discharged with a diagnosis of HF who did not have clear precipitants for renal dysfunction; bP<.0001. Krumholz H, et al. Am J Cardiol. 2000;85:1110-1113. 20 Raised Venous Pressure: A Direct Cause of Renal Sodium Retention GFR, mL/min 1.4 1.1 0.8 a High CVP significantly impairs GFR aP<.05 0.5 0 6.25 12.5 18.75 25 CVP, mm Hg vs baseline period 0 CVP, central venous pressure; GFR, glomerular filtration rate. Adapted from Firth JD, et al. Lancet. 1988;1:1033-1036. 21 Importance of Venous Congestion for Worsening Renal Function in ADHF Relative Contributions of CVP and CI to GFR at Time of Pulmonary Artery Catheter Removal P=.02 100 GFR, mL/min 80 60 40 20 0 High Cl / Low CVP 20% Low Cl / Low CVP 32% High Cl / High CVP Low Cl / High CVP 25% 23% Error bars represent 95% confidence interval (CI). Cutoff values for CI = 2.4 L/min/m2 and CVP = 8 mm Hg. CVP, central venous pressure; CI, cardiac index; GFR, glomerular filtration rate. 22 Reproduced with permission from Mullens W, et al. J Am Coll Cardiol. 2009;53:589-596. Tailoring Therapy Clinical Pearls ● Although the concept was ignored in the guidelines and in recent trial designs, targeting treatment to pathophysiology would be logical – Analogy: O2 is good for all pneumonia with hypoxia, but antibiotics must be tailored to the organism ● Similarly, although furosemide and/or nitrates may help all ADHF symptomatically, beyond acute reduction in pulmonary venous pressure, therapy should ideally target the cause of the decompensation Courtesy of Steven R. Goldsmith, MD. 23 Therapy: No new therapies approved since nesiritide Diuretics! Diuretics! Renal replacement Rx Vasodilators – Nitrates – Nesiritide – Nitroprusside Inodilators – Milrinone Inotropes – Dobutamine, dopamine Novel agents – Serelaxin Diuretics in Hospitalized Patients I IIa IIb III I IIa IIb III Patients with HF admitted with evidence of significant fluid overload should be promptly treated with intravenous loop diuretics to reduce morbidity. If patients are already receiving loop diuretic therapy, the initial intravenous dose should equal or exceed their chronic oral daily dose and should be given as either intermittent boluses or continuous infusion. Urine output and signs and symptoms of congestion should be serially assessed, and the diuretic dose should be adjusted accordingly to relieve symptoms, reduce volume excess, and avoid hypotension. Diuretics in Hospitalized Patients (cont.) I IIa IIb III I IIa IIb III The effect of HF treatment should be monitored with careful measurement of fluid intake and output, vital signs, body weight that is determined at the same time each day, and clinical signs and symptoms of systemic perfusion and congestion. Daily serum electrolytes, urea nitrogen, and creatinine concentrations should be measured during the use of intravenous diuretics or active titration of HF medications. When diuresis is inadequate to relieve symptoms, it is reasonable to intensify the diuretic regimen using either: a. higher doses of intravenous loop diuretics. b. addition of a second (e.g., thiazide) diuretic. The Hospitalized Patient Intensifying the Diuretic Regimen When diuresis is inadequate to relieve congestion, as evidence by clinical evaluation, the diuretic regimen should be intensified by using one of the following I IIa IIb III Higher doses of loop diuretics Adding a second diuretic (such as metolazone, spironolactone, or IV chlorothiazide) Continuous infusion of a loop diuretic Hunt SA, et al. Circulation. 2009;119:e391-e479. 27 Patients' Global Assessment of Symptoms during the 72-Hour Study-Treatment Period. Felker GM et al. N Engl J Med 2011;364:797-805. Kaplan–Meier Curves for the Clinical Composite End Point of Death, Rehospitalisation, or Emergency Department Visit. Felker GM et al. N Engl J Med 2011;364:797-805. Mean Change in Serum Creatinine Level. Felker GM et al. N Engl J Med 2011;364:797-805. Secondary End Points for Each Treatment Comparison. Felker GM et al. N Engl J Med 2011;364:797-805. Conclusions Among patients with acute decompensated heart failure, there were no significant differences in patients' global assessment of symptoms or in the change in renal function when diuretic therapy was administered by bolus as compared with continuous infusion or at a high dose as compared with a low dose. Diuretics in Hospitalized Patients (cont.) I IIa IIb III Low-dose dopamine infusion may be considered in addition to loop diuretic therapy to improve diuresis and better preserve renal function and renal blood flow. An approach to treating patients with acute heart failure who are diuretic resistant Maaten J M, et al. Nat Rev Cardiol. 2015 Mar;12(3):184-192. Vasodilators in AHF Mechanism of action – cGMP-mediated venous and/or arterial vasodilation (reduces preload and/or afterload) Advantages – Rapid symptomatic improvement – Relatively safe Disadvantages – – – – – Minimal effect in increasing cardiac output Hypotension, headache Tolerance/tachyphylaxis (frequent titration) Invasive monitoring, cyanide toxicity (nitroprusside) Unclear effect on hospitalization and mortality Hunt SA, et al. Circulation. 2009;119:e391-e479. 35 HFSA 2010 Practice Guideline ADHF — IV Vasodilators Recommendation 12.17 In the absence of symptomatic hypotension, IV nitroglycerin, nitroprusside, or nesiritide may be considered as an addition to diuretic therapy for rapid improvement of congestive symptoms in patients admitted with ADHF (Strength of Evidence = B) – Frequent blood pressure monitoring is recommended with these agents (Strength of Evidence = B) – These agents should be decreased in dosage or discontinued if symptomatic hypotension or worsening renal function develops (Strength of Evidence = B) – Reintroduction in increasing doses may be considered once symptomatic hypotension is resolved (Strength of Evidence = C) Lindenfeld J, et al. J Card Fail. 2010;16:e1-e194. 36 HFSA 2010 Practice Guideline ADHF — IV Vasodilators Recommendation 12.18 IV vasodilators (IV nitroglycerin or nitroprusside) and diuretics are recommended for rapid symptom relief in patients with acute pulmonary edema or severe hypertension (Strength of Evidence = C) Recommendation 12.19 IV vasodilators may be considered in patients with ADHF who have persistent severe HF despite aggressive treatment with diuretics and standard oral therapies – Nitroprusside (Strength of Evidence = B) – Nitroglycerine, nesiritide (Strength of Evidence = C) Lindenfeld J, et al. J Card Fail. 2010;16:e1-e194. 37 Nitrates vs Diuretics in Fulminant Pulmonary Edema Primary Outcome Predominant Isosorbide Dinitrate (n=52) Predominant Furosemide (n=52) P Value Died 1 (2%) 3 (6%) .61 Required mechanical intervention 7 (13%) 21 (40%) .0041 MI 9 (17%) 19 (37%) .047 Any adverse event 13 (25%) 24 (46%) .041 Cotter G, et al. Lancet. 1998;351:389-393. 38 Inotropes/Inodilators in ADHF Mechanism of Action – Increased cAMP via b-adrenergic receptors (dobutamine) or PDE inhibition (milrinone) – Increased myocardial contractility and peripheral vasodilation Advantages – Increased cardiac output and organ perfusion Disadvantages – – – – – Increased myocardial oxygen consumption Unpredictable hypotension (milrinone) Tolerance Increased arrhythmias Increased mortality Teerlink JR, et al. Heart Fail Rev. 2009;14:243-253. 39 HF Etiology and Response to Milrinone in ADHF (OPTIME-CHF) 1 0.98 Survival 0.96 0.94 0.92 Milrinone, ischemic Milrinone, nonischemic Placebo, ischemic Placebo, nonischemic 0.9 0.88 0.86 0 10 20 30 40 50 60 Days Reproduced with permission from Felker GM, et al. J Am Coll Cardiol. 2003;41:997-1003. 40 Avoiding Renal Failure Clinical Pearls ● Both persistent congestion and worsening renal failure are very poor prognostic features after treatment for ADHF ● Recent data may be tipping toward greater importance of decongestion, so long as worsening renal failure is transient ● Comparative trials of renal-sparing vs loop-diuretic based regimens are however limited at present ● In theory, decongestion without some of the adverse renal and neurohormonal effects of furosemide would be desirable Courtesy of Steven R. Goldsmith, MD. 41 Assessing Adequacy of Treatment Clinical Pearls ● Ideally, patients leave the hospital completely decongested, with normalized cardiac filling pressure and arterial pressure ● Registry and even trials data suggest we are not meeting that goal consistently ● We are not sure of how to assess the adequacy of decongestion in many patients, without direct measurement of filling pressures, and even that may not be completely satisfactory (ESCAPE trial) Courtesy of Steven R. Goldsmith, MD. 42 Use of Pulmonary Artery Catheterization: No Effect on Mortality and Hospitalization (ESCAPE) Cumulative Proportion 1.0 PAC + Clinical Assessment (n=206) Clinical Assessment Only (n=207) 0.8 0.6 0.4 0.2 0 30 60 90 120 150 180 Days Well (not dead or hospitalized) Reproduced with permission from The ESCAPE Investigators and ESCAPE Study Coordinators. JAMA. 2005;294:1625-1633. 43 Hyponatremia in ADHF 44 Hyponatremia Classification ● Depletional hyponatremia occurs due to loss of solute relative to total body water ● Dilutional hyponatremia occurs due to excess water relative to total body sodium (which may be normal in euvolemic states, or increased, in hypervolemic states) Verbalis JG. Best Pract Res Clin Endocrinol Metab. 2003;17:471-503. 45 Hyponatremia: Pathophysiology ● Dilutional hyponatremia is due primarily to excessive levels of circulating arginine vasopressin (AVP), the major hormone regulating total body water1 and the RAAS system ● In ADHF, hyponatremia is nearly always dilutional since total body volume is nearly always increased in this situation, meaning that excessive circulating AVP is the primary cause2 ● Reducing AVP levels or antagonizing the renal receptor for AVP are therefore the most rational approaches to treating hyponatremia in ADHF1,2 1. Adrogue HJ. Am J Nephrol. 2005;25:240-249. 2. Douglas I. Cleve Clin J Med. 2006;73(suppl 3):S4-S12. 46 AVP Levels Are Elevated in Patients With Hypo-osmolality and CHF 19.2 14.0 13.0 Plasma AVP, pg/mL No diuretics (n=14) Normal Range 15.0 12.0 4.0 3.0 Taking diuretics (n=23) 2.0 1.0 0.5 0.0 250 260 270 280 290 300 Plasma Osmolality, mOsm/kg of Water Reproduced with permission from Szatalowicz VL, et al. N Engl J Med. 1981;305:263-266. 47 Furosemide Accelerates LV Systolic Dysfunction placebo-treated (blue line) furosemide-treated animals (red line) p = 0.038 McCurley, J. M. et al. J Am Coll Cardiol 2004;44:1301-1307 P = 0.013 P < 0.05 Cosin J et al. Eur J Heart Fail. 2002; 4:507-13 Lopez B et al. JACC 2004; 43: 2028-35 Relation Between Dose of Loop Diuretics and Outcomes in a Heart Failure Population: Results of the ESCAPE Trial Hasselblad V et al. Eur J Heart Fail 2007; 9: 1064-9 My “cocktail” Constant infusion loop diuretic 5, 10 mg/hr with loading dose Slow to allow refill time from extracellular space Gentler on the kidney If significant peripheral (3rd space edema), add spironolactone – ½- 1 hr pre loop diuretic – Follow K carefully – Can increase to bid or tid if K is stable Add nitrates, oral, nitropaste or IV nitroglycerin. In outpatient, increases in ACEI/ARB, automatic decrease in daily diuretic – Address the RAAS increase Gracias!