Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
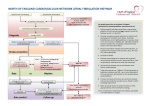
Atrial fibrillation What is it? AF is an arrhythmia is which electrical activity in the atria is disorganised The AV node receives more electrical impulses than it can conduct, and many are blocked, resulting in an irregular ventricular rhythm If untreated the ventricular rate averages 160-180bpm (or even lower) AF is the most common arrhythmia in clinical practice Prevalence doubles with each advancing decade from the age of 50 years AF doubles mortality rate Stroke risk is increased 6x and in AF with rheumatic heart disease 18x What causes it? Most common IHD, Hypertension, Mitral stenosis, Hyperthyroidism Cardiac &/or valve conditions Heart failure, rheumatic heart disease, pre-excitation syndromes (eg Wolff Parkinson White syndrome) Non cardiac conditions Lung cancer, acute infections Dietary and lifestyle factors Excess alcohol, excess caffeine, obesity How might AF present in GP? People with an irregular pulse +/ Asymptomatic Palpitations Chest pains Breathlessness Syncope / giddiness Reduced exercise tolerance, malaise or polyuria A potential complication of AF such as stroke, TIA or heart failure Diagnosis Manual pulse palpation very sensitive but specificity less good ECG No P waves Chaotic baseline Irregular ventricular rate Ventricular complexes look normal unless there is a conduction defect If paroxysmal AF suspected AF and 12 lead ECG is normal then arrange ambulatory ECG Bloods CXR Bloods? FBC – exclude anaemia U+Es, bone profile, glucose – exclude electrolyte disturbances which may precipitate AF LFTs and clotting – suitability for warfarin CXR – lung cancer, detect heart failure When to urgently refer Pulse >150bpm &/or low BP (systolic < 90 mmHg) Loss of consciousness, severe dizziness, ongoing chest pain or increasing breathlessness Complication of AF Stroke, TIA, acute HF Key priority ― Detection and diagnosis NICE clinical guideline 36, June 2006 Case detection Assessment O R Ratecontrol Rhythmcontrol Follow-up Follow-up Referral An ECG should be performed in all patients, whether symptomatic or not, in whom AF is suspected because an irregular pulse has been detected Classification Paroxysmal Intermittent and recurrent, but terminates spontaneously (35-65% of all cases) Reverts to sinus rhythm within 7 days Persistent Does not convert spontaneously, but may be converted electrically or by the use of drugs Lasts over 7 days and less than a year Permanent Long standing and resistant to cardioversion. Also term for long-standing AF (>1year) where cardioversion has not been attempted Complications Stroke and thromboembolic events 6x greater risk Heart failure Tachycardia-induced cardiomyopathy Critical cardiac ischaemia Poorer life quality Prognosis Mortality from AF up to 2x general population Linked to severity of underlying heart disease (eg heart failure, cardiomyopathy or myocardial ischaemia) Acute onset AF Requires immediate hospitalisation and urgent intervention Those at highest risk include: Ventricular rate >150bpm Ongoing chest pain Critical ischaemia Treatment options Antithrombotic therapy Treatment options – antithrombotic therapy Warfarin is more effective but balance this against a higher risk of a major bleed Warfarin reduces relative risk of all strokes vs placebo by 60% Aspirin reduces relative risk of all strokes vs placebo by 20% Actual benefit is based on persons baseline risk Key priority ― Assess for risk of stroke & thromboembolism NICE clinical guideline 36, June 2006 Case detection Assessment O R Ratecontrol Rhythmcontrol Follow-up Follow-up Referral - Use the stroke risk Stratification algorithm to assess risk - Use antithrombotic therapy as appropriate - Initiate antithrombotic therapy without minimal delay in patients newly diagnosed with AF Assess for risk of stroke and thromboembolism NICE clinical guideline 36, June 2006 Determine stroke/thromboembolic risk High risk: • Previous ischaemic stroke/TIA or thromboembolic event • Age >75 with hypertension, diabetes or vascular disease • Clinical evidence of valve disease, heart failure, or impaired left ventricular function on echocardiography Moderate risk: Low risk: • Age >65 with no moderate or high risk factors no high risk factors • Age <75 with hypertension, diabetes or vascular disease • Age <65 with Patients with AF NICE clinical guideline 36, June 2006 Determine stroke/thromboembolic risk High risk Consider anticoagulation Contraindications to warfarin? NO Warfarin, target INR = 2.5 (range 2.0 to 3.0) Moderate risk Low risk Consider anticoagulation or aspirin Aspirin 75 to 300 mg/day if no contraindications YES Reassess risk stratification whenever individual risk factors are reviewed CHADS2 Congestive heart failure = 1 Hypertension (or treated hypertension) = 1 Age older than 75 years = 1 Diabetes mellitus = 1 Previous Stroke or TIA = 2 Treat with aspirin if total score is 0 or 1 Use warfarin if score is 2 or more Possible questions? How do the harms and benefits of aspirin compare? How does low dose warfarin compare with adjusted dosing? What about using clopidogrel instead of aspirin? How do the harms and benefits of aspirin compare? Harms from aspirin Take 1000 patients 6 will have a major extracranial bleeding in 1 year anyway If they take aspirin 1 more will have a bleed caused by aspirin Harms from warfarin Take 1000 patients 6 will have a major extracranial bleeding in 1 year anyway If they take warfarin 3 more will have a bleed caused by warfarin Anticoagulation Assessment of bleeding risk should be part of clinical assessment prior to starting anticoagulation Benefits and potential risks of anticoagulation should be discussed Aim for INR between 2 and 3 Benefits of aspirin (low risk eg 1% per year) Take 1000 patients 10 will have a stroke in 1 year (1%) If aspirin is taken 8 will have a stroke 2 will be prevented from having a stroke Benefits of warfarin (low risk eg 1% per year) Take 1000 patients 10 will have a stroke in 1 year (1%) If warfarin is taken 4 will have a stroke 6 will be prevented from having a stroke Benefits of aspirin (moderate risk eg 3.5% per year) Take 1000 patients 35 will have a stroke in 1 year (3.5%) If aspirin is taken 28 will have a stroke 7 will be prevented from having a stroke Benefits of warfarin (moderate risk eg 3.5% per year) Take 1000 patients 35 will have a stroke in 1 year (3.5%) If warfarin is taken 14 will have a stroke 21 will be prevented from having a stroke Benefits of aspirin (higher risk eg 6% per year) Take 1000 patients 60 will have a stroke in 1 year (6%) If aspirin is taken 48 will have a stroke 12 will be prevented from having a stroke Benefits of warfarin (higher risk eg 6% per year) Take 1000 patients 60 will have a stroke in 1 year (6%) If warfarin is taken 24 will have a stroke 36 will be prevented from having a stroke How does low dose warfarin compare with adjusted dosing? Adjusted dosing is better with no obvious increased harms What about using clopidogrel instead of aspirin? No evidence of significant benefit Clopidogrel alone (within its unlicensed indications) is recommended for people who are intolerant of low dose aspirin and either have: Experienced an occlusive vascular event Have symptomatic PAD Aspirin intolerance is either: Proven hypersensitivity to aspirin containing medicines History of severe dyspepsia induced by low dose aspirin Treatment options Rate or rhythm control Treatment for persistent AF 2 treatment options Rate control involves the use of chronotropic drugs or electrophysiological / surgical interventions Rhythm control involves the use of electrical or pharmacological cardioversion for persistent AF, or suppression of recurrent (eg paroxysmal) AF There is a need for appropriate antithrombotic therapy if rhythm control is chosen NICE clinical guideline 36, June 2006. Quick Reference Guide Treatment for paroxysmal AF Patients can be highly symptomatic 3 main aims of Rx are to : Suppress paroxysms of AF and maintain sinus rhythm Control heart rate during paroxysms of AF Prevent complications Treatment strategies include out of hospital initiation of antiarrhythmic drugs : ‘pill in the pocket’ approach Patients with paroxysmal AF carry the same risks of stroke and thromboembolism as those with persistent AF Key priority ― choosing the most effective treatment NICE clinical guideline 36, June 2006 Case detection Assessment O R Ratecontrol Rhythmcontrol Follow-up Follow-up Referral -Some patients with persistent AF will satisfy criteria for either an initial rate or rhythm control strategy -Indications for each Rx are not mutually exclusive -Involve the patient in the treatment decision -Take comorbidities into account -Antithrombotic therapy should always be used Rate control What is it? Control the ventricular rate (AF remains) How is it done? Drugs that block AV node conduction (B blockers, Ca channel blockers, digoxin) Why is it done? Reduce symptoms and myopathy Prevention of embolism & cardiomyopathy Advantages? As effective as rhythm control Lower risk of adverse events Lower cost Less hospitalisation Avoids antiarrhythmics Disadvantages? May not remove symptoms Requires anticoagulation Risk of tachycardiomyopathy Atrial remodelling (permanent) When may it be appropriate? First line particularly in elderly with minimal symptoms Patients at high risk of stroke Rate control strategy Try rate control 1st for patients with persistent AF : Over 65 With CHD With contraindications to antiarrhythmic drugs Unsuitable for cardioversion Without CCF Rhythm control What is it? Restore and maintain sinus rhythm How is it done? Electrical / drug conversion (plus maintenance antiarrhythmic drugs) Why is it done? Reduce symptoms and myopathy Prevention of embolism & cardiomyopathy Advantages? Better exercise tolerance Improved haemodynamic function Reverse modelling? Less need for, but still requires, antithrombotic treatment Disadvantages? Difficult to maintain in long term High adverse event rate More hospitalisation High rates of recurrence When may it be appropriate Young patients New onset AF Where rate control ineffective or symptoms remain Rhythm control strategy Try rhythm control 1st for patients with persistent AF : Who are symptomatic Who are younger Presenting for the 1st time with lone AF Secondary to a treated / corrected precipitant With CCF What about restoring sinus rhythm? DC cardioversion restores sinus rhythm in >80% In AF of recent onset drugs have a success rate of 40-90% Sinus rhythm at 1y is maintained in 30% without antiarrhythmic therapy but in 50% with such therapy Follow up and referral Follow up after cardioversion should be at 1 month and then tailored to the individual Reassess the need for anticoagulation at each review Referral for further specialist intervention should be considered in those : In whom pharmacological therapy has failed With lone AF With ECG evidence of any underlying electrophysiological disorder