Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
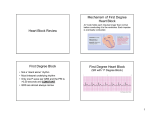
Name That Rhythm EMT-Intermediate W06 And you thought we wouldn’t review….. Heart A & P • • • • • Location Pieces, Parts Important Vessels Electrolyte Role Pulling apart waveforms Valves & Vessels Review of Important Vessels The Components • SA Node • Internodal Pathways • AV Junction • AV Node • Bundle of His • L & R Bundle Branch • Purkinje Network • Purkinje Fibers The Route Sino Atrial Node • The Natural “Pacemaker” – Connects directly to atrial fibers .04 Sec • Fires 60-100 times per minute • Wavelike Atrial Depolarization • The P-Wave 0.20 Seconds per 5 Boxes .04 Sec .04 Sec .04 Sec .04 Sec P-Wave QWave P-R Interval AV Junction • Receives impulses from SA Node via the Atrial Cells – An electrical funnel – Impulses hit at various times – Causes delay • PR-I – Susceptible to blockage • Path from A to V – Delivers impulse to the AV Node Atrio-Ventricular Node • Lies between the Atria and Ventricles • Collects impulses from above • Stimulates Ventricles • If unstimulated – Intrinsic rate 40-60 Bundle of His / Left and Right Bundle Branches • Distributes Impulses from the Node • “The Ventricular Messengers” Purkinje Network/Fibers • Direct connection with ventricular tissue • Intrinsic rate 20-40 if unstimulated T-Wave P-Wave P-R Interval QRS Complex Electrical Conduction System • Sympathetic-Thoracic/Lumbar Nerve – Norepinephrine • HR, Contractility • Parasympathetic-Vagus Nerve – Acetylcholine • HR (Valsalva) • Chronotropic-HR • Inotropic-Contraction Electrical Conduction System • Na+ in & K+ out = Depolarization • K+ in & Na+ out = Repolarization – Imbalances in K+ or Na+ • Effects Automaticity & Conduction • Hypo & hyperkalemia affects irritability • Ca++ - Depolarization and Contraction – Affects Contractility – Hypo & Hypercalcemia effects contractile force Phases • Phase 0 – Rapid Depolarization – Reached max potential -90mV – Fast Na+ Channels Open – Cell now positive +25mV • Phase 1 – Early Rapid Repolarization – Fast Na+ Channels Close – K+ still being lost – MP approaching 0mV • Phase 2 – Prolonged Slow Repolarization – – – – Plateau Phase Muscle finishing contraction Beginning to relax MP staying close to 0mV Phases • Phase 3 – End of Rapid Repolarization – K+ returns to inside – Cell returns to -90mV – Almost ready • Phase 4 – Na+ - K+ Pump turns on • Sends Na+ out • Brings K+ in • Ready to do it all over again now Refractory Periods Excuse me!!! I hate to interrupt again, but, who cares??? • Absolute Refractory Period – Polarity of cell prohibits depolarization • Relative Refractory Period – Cell is returning to ready state for depolarization – Impulse now is BAD!!! • R on T Phenomenon – Causes VT & VF – Treated with defibrillation • Can be caused by: – Frequent PVC’s – EMT-P not pushing the “sync” button QRS Complex Lead Considerations • $25,000 mVoltmeter – Lead Views: • 1 – Lateral • 2 – Inferior • 3 – Inferior The Six Step Approach • • • • • • What is the Rate? Is the Rhythm Regular? Are there P-Waves? Is the P-R Interval Normal? Is the QRS Complex Normal? Is There a P-Wave for Every QRS? Describe What You’ve Found!!! • • • • IN GENERAL (underlying rhythms)!!! What are the abnormalities? Does it originate in the Sinus Node? Does it follow through from the Atria to the ventricles? Are there abnormal delays? • What are the exceptions to the underlying rhythm? (Describe those also) Normal Sinus Rhythm • • • • • • Rate: 60 - 100 Regularity: Very P-Waves: Present and Normal P-R I: 0.12-0.20 sec QRS: 0.04-0.12 sec and Normal Married: 1 P: 1 QRS, no extras or shortages Sinus Arrhythmia Rate: 60 - 100 Regularity: Irregular P-Waves: Present and Normal P-R I: 0.12-0.20 sec QRS: 0.04-0.12 sec and Normal Married: 1 P: 1 QRS, no extras or shortages Sinus Tachycardia Rate: Over 100 Regularity: Regular P-Waves: Present and Normal P-R I: 0.12-0.20 sec QRS: 0.04-0.12 sec and Normal Married: 1 P: 1 QRS, no extras or shortages Sinus Bradycardia Rate: Less than 60 Regularity: Regular P-Waves: Present and Normal P-R I: 0.12-0.20 sec QRS: 0.04-0.12 sec and Normal Married: 1 P: 1 QRS, no extras or shortages Atrial Fibrillation Rate: Usually tachy Regularity: Irregular (Irregularly irregular) P-Waves: Not Discernible P-R I: Undeterminable QRS: 0.04-0.12 sec Married: Undeterminable Atrial Flutter Rate: Usually tachy Regularity: Atria Regular • Ventricles May be Irregular P-Waves: Sawtooth Pattern 2:1, 3:1, 4:1... P-R I: 0.12-0.20 sec on conducting beat QRS: 0.04-0.12 sec Married: P-waves outnumber QRS (Picket fence) (Paroxysmal) Supra Ventricular Tach Rate: 140-220 Regularity: Regular P-Waves: Usually falls within the QRS-T complex (not visible) P-R I: Shorter than 0.12, or absent QRS: 0.04-0.12 sec and Normal Married: Undeterminable SVT • WPW – Usually based on Hx. – Delta wave on Q – Shortened PR-I – No Verapamil – Accessory Path use increase 1st Degree Heart Block Rate: 60 - 100 Regularity: Very P-Waves: Present and Normal P-R I: Longer than 0.20 sec QRS: 0.04-0.12 sec and Normal Married: 1 P: 1 QRS, no extras or shortages 2nd Degree Heart Block (Type 1) Wenkebach Rate: Can be Normal, or usually brady Regularity: Irregular P-Waves: Present and Normal P-R I: Lengthens until beat is dropped QRS: 0.04-0.12 sec and Normal Married: P-wave present on conducting beats, increased delay causes missed QRS 2nd Degree Heart Block (Type 2) Mobitz II Rate: Less than 60 Regularity: Irregular P-Waves: Present, 2:1, 3:1, 4:1 P-R I: 0.12-0.20 sec on conducting beat QRS: 0.04-0.12 sec, may begin to widen Married: P-wave for every QRS and extras depending on conduction ratio 3rd Degree Heart Block (CHB) Complete Heart Block Rate: Ventricular Rate 40-60 Regularity: Atria-Regular • Vent-Regular P-Waves: Present and Normal P-R I: Atria independent of Ventricles QRS: Usually greater than 0.12 sec Married: P-waves completely unrelated to QRS Complexes. Complete Heart Block Junctional Rhythm Rate: 40-60 Regularity: Regular P-Waves: Inverted, Retrograde or Absent P-R I: Shortened or absent QRS: 0.04-0.12 sec Married: P-wave for every QRS, sometimes not visible Junctional Junctional Accelerated Rhythm Rate: 60-100 Regularity: Regular P-Waves: Inverted, Retrograde or Absent P-R I: Shortened or absent QRS: 0.04-0.12 sec Married: P-wave for every QRS, sometimes not visible Junctional Tachycardia Rate: 100-140 Regularity: Regular P-Waves: Inverted, Retrograde or Absent P-R I: Shortened or absent QRS: 0.04-0.12 sec Married: P-wave for every QRS, sometimes not visible Ventricular Tachycardia We’ll look at Torsades de Pointes in Lab Rate: 100-220 Regularity: Regular P-Waves: None P-R I: None QRS: Greater than 0.12 sec Married: NO Ventricular Tachycardia Ventricular Fibrillation Rate: No ventricular rate Regularity: Irregular P-Waves: No P-R I: No QRS: No, unorganized ventricular baseline Married: No Ventricular Fibrillation Asystole Rate: 0 Regularity: N/A P-Waves: None P-R I: N/A QRS: None Married: No (verify a second lead) Asystole Agonal / Idioventricular Rate: 20-40 Regularity: Irregular P-Waves: None P-R I: N/A QRS: Wider than 0.12 sec Married: NO (a dying heart) Idioventricular • Less regular than this! Exceptions / Disruptions • • • • Premature Ventricular Contractions Premature Atrial Contractions Bundle Branch Blocks Pacer Considerations (Atrial, Ventricular or Both) Premature Ventricular Contractions • Wide, Bizarre QRS Complex • Always identify the underlying rhythm first • Can appear in couplets, triplets, short runs of V-Tach, bigeminy and trigeminy • Can be uni-focal or multi-focal • Caused by random firing within the ventricles • Not accompanied by a P-wave PVC’s PAC’s • P-QRS Complex appearing in an unexpected location • Caused by a stimulus from within the Atria, but not from the SA Node PJC Bundle Branch Block • Any rhythm having a BBB will have a widened twin peaked R-Wave Paced Rhythms • Patients may have various types of pacemakers • Atrial • Ventricular • Both • Vertical spike on monitor is an indicator Paced Rhythms Various Artifact • 60 Cycle Interference • Loose Leads/Moving Ambulance In Summary • Really Cool Physiology!!! • GENERAL RULES to Interpretation – Applicable to 3 – lead monitoring • Practice, Practice, Practice… • Remember the rules, NOT how it looks coming from one patient or one rhythm generator!!! Sources – In order of preference • Many of the pictures and info from: – Flip and See ECG, 2nd Edition • Cohn/Gilroy-Doohan – A great resource – Paramedic Paramedic Textbook, Revised 2nd Edition • Mick J. Sanders, Mosby – ECG’s Made Easy, 2nd Edition • Barbara Aehlert, RN, Mosby – Basic Dysrhythmias, Interpretation and Management, 3rd Edition • Robert J. Huszar, Mosby