Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Aortic stenosis wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Jatene procedure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Atrial fibrillation wikipedia , lookup
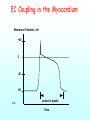
Pumps Positive and negative pressure operation Hearts and accessory pumps Valves: Devices for Unidirectional Flow Opened hi gh p ressu re Closed mu scl e fo rce hi gh pre ssure mu scl e fo rce Functional Aspects of Hearts Force generation (“myocardium”) Directionality (valves) Coordination Myocardial and Nodal Cell Potentials Membrane Potential, mV +40 typical myocardial cell typical SA nodal cell 0 -40 resting membrane potenital threshold threshold -80 maximum diastolic potential knp Time spontaneous depolarization, also called the pacemaker potential Preferential Bioelectrical Pathways SA Node Bachmann's Bundle AV Node LA RA RV knp Purkinje FIbers LV Left and Right Bundle Branches (Bundles of His) EC Coupling in the Myocardium Membrane Potential, mV +40 0 -40 -80 knp period of systole Time Atrial Conduction The AV Node Atrial Side A V Node Ventricular Side knp atrial myocardium (fast conduction) Nodal Cells Bundles of His (fast conduction) Ventricular Conduction Autonomic Effects on Chronotropicity: 1. Parasympathetic Effects Parasympathetic (mediated via X cranial (vagus) nerve) Receptor: muscarinic (inhibitory) Agonists -- ACH, muscarine, carbachol -- all have negative chronotropic effects and slow rate from what it would have been Antagonists: atropine -- block negative chronotr. effect. Autonomic Effects on Chronotropicity: 2. Sympathetic Effects Sympathetic (mediated via “accelerator” nerve and epinephrine). Receptors: 1 (NE from accelerator) and 1epinephrine. 1 • Agonists: NE and phenylepherine -- both have weak positive chronotropic effects. • Antagonist: phenoxybenzomine has a very slight negative or no chronotropic effect. 1 • Agonists: E, isoproterenol (isupryl) and ephedrine all have strong positive chronotropic effects. • Antagonists: propranolol (inderal) -- blocks positive chronotr. effect. Nodal Cells and Chronotropicity Fick’s Principle for Determination of Cardiac Output Is there a non-invasive way to determine cardiac output? V O2 Q(CaO2 CvO2 ) VO 2 Q (CaO2 CvO2 ) The Frank-Starling Law of the Heart Systolic Pressure, Force, or Tension knp Diastolic Pressure, Tension, Force, or Length The Autonomic NS and Ionotropic Effects Parasympathetic -- no direct effect, indirect effect only (covered later). Sympathetic -- strong ionotropic effect (think about what happens when you are scared). • Therefore, alpha- & beta-agonists (e.g. epinephrine and isoproterenol) will have a strong positive ionotropic effect (and increase electrical excitability). • β -blockers (propranolol (inderal)) will generally cause a decrease in contractile force and stroke volume (and electrical excitability) as they block the E that is normally present. The Effect of Epinephrine on Contractility Systolic Pressure knp increasing sympathetic stimulation Diastolic Pressure Cardiac Work Loop E 150 rapid ejection 125 Pressure, mHg 100 F D 75 50 isovolumic contraction isovolumic relaxation C A 25 knp 50 75 Ventricular Volume B 100 125 isovolum. atrial contract. rapid systole ejection 120 isovolum. rapid relax. reduced ventric. ejection filling aortic semilunar closes aortic semilunar opens Pressure (mm Hg) reduced ventric. filling aortic pressure 80 left ventricular pressure 40 mitral valve closes mitral valve opens left atrial pressure 0 4 Aortic Blood Flow (L/min.) 2 0 Ventr. Vol. (ml) 38 32 26 20 1 4 Heart Sounds 2 3 R EKG T P P Q 0 knp, after Berne and Levy, Fig. 29-12, Physiology. Mosby, 1983 S 0.4 Time (seconds) 0.8 Summary: the Timing of Mechanical and Electrical Events