Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
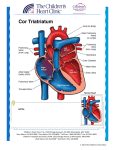
“It is of the highest importance in the art of detection to be able to recognize out of a number of facts, which are incidental and which vital. Otherwise your energy and attention must be dissipated instead of being concentrated“ Sherlock Holmes, in The Regitate Puzzle Fact: Ca++ 5.5, Mg++ 5.2 Hypocalemia, Cyanotic congenital heart disease – could this be DiGeoge’s Syndrome?? (truncus with parathyroid Hypoplasia) “When a fact appears to be opposed to a long train of deductions, it invariably proves to be capable of bearing some other interpretation.” Sherlock Holmes in A Study in Scarlet Summary: A middle aged, African-American woman presented with profound hypoxemia, cor pulmonale (pulmonary hypertension and right ventricular failure) and severe left ventricular dysfunction, with laboratory evidence of myocardial injury and coagulopathy. She died suddenly with a cardiopulmonary arrest. So, what are the key features of her presentation, what do we know, and what would we like to know? The presence of severe hypoxemia that does not correct with the administration of 100% oxygen is diagnostic of right-to-left shunting, either across the heart or the lungs. History: 1). No past medical history – presenting in 5th decade; * argues against cyanotic congenital heart disease (Tetralogy of Fallot, Transposition of the Great Vessels) * could use a few more details regarding childhood activity level and the pace of her functional decline History: 2). Presents with 2 weeks of LE edema, but no PND or orthopnea; * R heart failure >> L heart failure * did this really only develop over 2 weeks? (doubtful) * what happened 2 weeks ago to push her over the edge? 3). Pagophagia (the specific eating of ice); * strongly suggestive of iron deficiency * can also be cultural, particularly in AA 4). Ingestion of both Vitamin E and cod liver oil; * raise the possibility of Vitamin E intoxication * might at least be complicating the apparent hepatic dysfunction History: 5). Surgery at age 30; * any details from that admission (ECG, HGB, etc.)? 6). No mention is made of children or pregnancies; * often poorly tolerated by patients with Congenital HD 7). History of “heart murmur” and possible rheumatic fever; * was murmur louder in the past than presently? (common in initial L-R shunting with progressive PH) * some murmurs are very distinctive and usually precipitate a work-up: harsh murmur of a restrictive VSD with thrill; continuous or “machinery” murmur of a PDA; ASDs are less specific and may be harder to hear, as would be a non-restrictive VSD, or Ebstein’s anomaly (with ASD) History: 7). History of “heart murmur” and possible rheumatic fever; * “rheumatic fever raises possibility of mitral stenosis, though such severe pulmonary hypertension with R-L shunting would be very unusual in rheumatic MS, unless there were other concomitant cardiac defects. 8). History of hair loss, constipation and fatigue; * suggestive of hypothyroidism * also consistent with iron deficiency. Physical Exam: 1). Vital signs: pulse 106, mild tachypnea (SpO2 77%); * tachycardia makes hypothyroidism unlikely; * absence of respiratory distress despite marked desaturation emphasizes chronicity of condition 2). Jugular venous distention, peripheral edema, clear lungs; * right heart failure >> left heart failure 3). Clubbing and cyanosis; * reflects chronic, severe hypoxemia, BUT; * what about central cyanosis - ? blue lips; * are upper (right and left) extremities similarly clubbed and cyanotic compared to LE? * these may give clues as to the site of the shunt! Physical Exam: 4). Cardiac exam: only soft systolic ejection murmru; * non-restrictive VSD may be quiet * murmurs may become quiet as R-L shunt predominates; * no mention is made of S1 (split and loud in Ebstein’s anomaly, or S2 (widely split and fixed in ASD) * ? thrill (VSD), RV heave (pulmonary htn) * ? change with respiration (TR) Laboratory Data: 1). HGB 15.3/HCT 47; * should be much higher in patient with severe, chronic hypoxemia and Eisenmenger’s syndrome; * may reflect the underlying iron deficiency? * has she undergone phlebotomy? * MCV is high, but could reflect mixed deficiency * What is the serum iron, and ferritin? 2). Mild elevation of LFTs, INR, slightly decreased Alb; * probably reflects hepatic congestion and cor pulmonale 3). Very high D Dimer; * ? presence of thrombophlebitis (DVT); * also elevated in any systemic illness with incr. fibrin * raises possibility of embolic events (heart, CNS) 4). Mild renal insufficiency; * probably due to impaired renal perfusion; Laboratory Data: 5). TSH normal; * makes hypothyroidism unlikely, though could have central abnormality – what’s the freeT4?; 6). Marked elevation of BNP; * consistent with biventricular failure 7). Elevated troponin (34); * suggests the presence of myocardial injury * can be elevated in pulmonary embolus, though not usually this high (and excluded by CT angio); * not much data on chronic right heart failure * doubt acute plaque rupture and typical CAD, but could reflect embolus down a coronary artery Laboratory Data: 8). Blood Gasses: 35/21/7.43 on 4l, 42/24/7.42 on 100%; * profound hypoxemia * modest respiratory alkalosis * essentially normal pH – reflects effective renal compensation, or superimposed metabolic acidosis Laboratory Data: 8). Blood Gasses: 35/21/7.43 on 4l, 42/24/7.42 on 100%; * profound hypoxemia * modest respiratory alkalosis * essentially normal pH – reflects effective renal compensation, or superimposed metabolic acidosis So what can cause hypoxemia of this magnitude: Alveolar hypoxia – altitude, intrinsic pulmonary disease, pulmonary edema with alveolar flooding V/Q mismatch (physiological dead space) – pulmonary hypertension, pulmonary embolus ** Right to left Shunt – intrapulmonary (pulmonary a-v malformation), or intracardiac Normal Heart Atrial Septal Defect (Secundum) Ventricular Septal Defect (Membranous) Ebstein’s Anomaly Patent Ductus Arteriosus Aortic pulmonary Window Eisenmenger’s Syndrome Other Data: 1). ECG sinus tach, RBBB, ? right axis; * axis provides evidence for site of lesion, particularly if ASD: right axis – secundum; left axis – primum junctional or low atrial rhythm – sinus venousus * make sure not hidden atrial flutter * negative p waves in Ebstein’s, also accessory pathways * ? ST segments with elevated troponin 2). Chest X-ray – cardiomegaly, no pulmonary edema; * right or left ventricular/atrial enlargement?; 3). CT angiogram – pruning, no pulmonary embolus; * pruning of pulmonary vessels typical with Eisenmenger’s; * confirms right atrial and biventricular enlargement * ? “low density enhancement” -- ? tumor, ? incidental finding, ? thrombus Other Data: 4). Echocardiogram – should be definitive test; a). It shows: * severe RA and RV enlargement * severe pulmonary hypertension These are consistent with chronic left to right shunting with the development of Eisenmenger’s syndrome – would be expected regardless of the site of the shunt. * severe left ventricular hypokinesis This would be unexpected for a shunt at the atrial level, and argues for a shunt that also overloads the LV (VSD, PDA, aortopulmonary window). If wall motion abnormalities are segmental, could reflect coronary emboli with subsequent MI. Other Data: 4). Echocardiogram – should be definitive test; a). It doesn’t show (or doesn’t say…): * clear evidence of ASD, VSD, or Ebstein’s Anomaly * any evidence of rheumatic mitral valve disease * left atrial enlargement, cor-triatriatum It might be possible to miss some lesions on a TTE, particularly at the atrial level (especially sinus venosus defects). However a large VSD, or Ebstein’s should be manifest, as would RHD. If not missed, it suggests that the lesion is outside of the heart itself, such as PDA, or aortopulmonary window. A TEE may be more sensitive… Other Data: 5). Cardiac Catheterization – pulmonary htn (70/40), elevated PCW pressure (43 mmHg), low cardiac output; * PCW seems very high, particularly with PAD only 40 mmHG. This makes transpulmonary gradient normal? Is this measurement correct? * was LVEDP measured as well as PCW at cath? * what about step-up in oxygen saturation? * was a Qp/Qs calculated? * magnitude of both L-R and R-L shunting should have been measured during cath * was a coronary angiogram done to look for emboli? * was a pulmonary angiogram or aortogram performed? Hospital Course: Sudden death due to cardiopulmonary arrest with PEA * unfortunately, very common with paradoxical emboli in in patients with Eisenmenger’s syndrome – could be innocent air emboli from a peripheral IV, or more dramatic thromboembolic event from a DVT. ** NEED TO USE AIR FILTERS ON ALL IV LINES AND USE EXTRAORDINARY CARE TO PREVENT PARADOXICAL EMBOLI DURING IV FLUSHES OR INFUSIONS. Other considerations: * infiltrative diseases affecting right and left ventricles (sarcoid, hemochromatosis) * cardiac tumors, including unusual lymphomas * inflammatory diseases (such as lupus) causing pulmonary hypertension, myocarditis, and pericardial effusion But I couldn’t figure out how to get severe hypoxemia and right to left shunting out of these disorders. So…. “It is a capital mistake to theorize before one has data. Insensibly one begins to twist facts to suit theories, instead of theories to suit facts. “ Sherlock Holmes, in A Scandal In Bohemia “There is nothing more stimulating than a case where everything goes against you.” The Hound of the Baskervilles CYANOTIC HEART DISEASES: Increased pulmonary circulations: •Complete transposition of the great arteries •Double outlet right ventricle •Taussig-Bing syndrome •Pulmonary arteriovenous fistula •Total anomalous venous return •Truncous arteriosus (type I, II and III) •Hypoplastic left ventricular syndrome: Aortic atresia Hypoplastic aortic artery Mitral valve atresia CYANOTIC HEART DISEASES: Normal pulmonary circulation or diminished pulmonary circulation: •Tetralogy of Fallot •Tricuspid atresia •Hypoplastic right ventricle •Ebstein anomaly •Pulmonic stenosis or atresia with ASD •Single ventricle with pulmonic stenosis •Eisenmenger syndrome •Truncous arteriosus (type IV) Transposition great arteries Patent ductus arteriosus Aortic pulmonary Window Eisenmenger’s Syndrome