Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
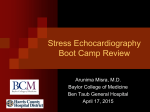
Stress Testing Source Elstead and experience STRESS TESTING: INDICATIONS 1. Precordial chest pain 2. Determine prognosis and severity of disease 3. Evaluation of arrhythmia 4. Evaluation of functional capacity and make exercise prescription. 5. Evaluate congenital heart disease i.e. shunts right-sided pressures STRESS TESTING: ABSOLUTE CONTRAINDICATION • Patient with acute MI • Patient with acute myocarditis or pericarditis • Patient with unstable progressive angina • Patient with rapid ventricular and atrial arrhythmias • Patient with 2nd and 3rd degree AV block • Acutely ill patient ie with infection, hyperthyroidism or severe anemia STRESS TESTING: RELATIVE CONTRAINDICATION • • • • • • • Aortic stenosis Hi-grade LVOT Suspected left main equivalent Severe hypertension 240/130 (Gracin: max 180) Severe ST depression at rest and history of angina Congestive heart failure – rales, edema AAA (adenosine most forgiving type of stress test) STRESS TESTING: WHEN TO TERMINATE THE EXERCISE TEST * Blood pressure or heart rate drops * Hypertension - 220 systolic or 110 diastolic especially if headache or visual changes * Severe ST depression i.e. 2mm in 2 contiguous lead * Patient has reached or exceeded the predicted maximum heart rate (need 85% nuclear 15-20 bpm over 85% for stress echo) * VT or runs of three or more * Atrial tachycardia, atrial fibrillation, or atrial flutter * 2nd or 3rd degree heart block * Angina pain * Dyspnea, faint, fatigue * Muscular pain of arthritis and claudication * Patient looks vasoconstricted – pale and clammy ST ABNORMALITIES upsloping 2mm upsloping ST depression at .08 sec after the J point (the tail end of QRS complex) horizontal 1mm horizontal ST depression downsloping 1mm downsloping ST depression ST DEPRESSIONS ST depression distribution does not correlate to coronary territory at risk. ST depressions are particularly specific on Adenosine and dipyridamole stress but less specific on dobutamine protocols. ST depressions are often falsely positive for ischemia with hypertension, digoxin, hypokalemia, and women. ST ELEVATIONS ST elevations reflect transmural ischemia and are significant in exercise, adenosine stress and DO CORRELATE to coronary territory at risk. The exception is Dobutamine, which often has ischemic changes not strictly correlated to ischemia. T-WAVE INVERSIONS T-Wave inversions are not specific and you do not need to wait until they return to normal before phasing out of the study. BRUCE PROTOCOL Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6 Stage 7 0-3 min 3-6 min 6-9 min 9-12 min 12-15 min 15-18 min 18-21 min 1.7 mph 2.5 mph 3.4 mph 4.2 mph 5.0mph 5.5 mph 6.0 mph 10% grade 12% grade 14% grade 16% grade 18% grade 20% grade 22% grade 5.0 Mets 6.8 Mets 9.4 Mets 13.3 Mets 16.6 Mets 19.5 Mets 22.7 Mets Mets are defined as: Metabolic equivalents + Multiples of 02 consumption of 3.5 ml/kg/min by a person in the sitting position. Describes functional capacity. Rate pressure product = Max HR x Max SBP (25,000 is a good effort) Useful if Hr is low and SBP is high. Modified Bruce: 2 minute intervals ½ stages Speed is constant grade increases. Naughton Protocol: 2 minute interval at 2 mph with grade changes 0%, 3.5%, 7%, 10.5%, 14%, 17.5%, 20% Bicycle Protocol Upright and Reclined Reclined is harder physically as legs are above the heart level. We do upright. Can watch RVSP rise with exercise. Start at 25 watts 60 rpm increase by 25 watts usually to 125 watts. Goal - still 85% max HR. Use a Dobutamine format on the echo machine. ADENOSINE/DIPYRIDAMOLE (PERSANTINE) Adenosine Protocol •140 mcg/kg/min for 6 minutes and inject MIBI at 3 minutes •Can do 4 minute and inject MIBI at 2 minutes and spare the patient the misery. Adenosine and Dyperidamole - vasodilatory drugs Normal vessels dilate while atherosclerotic vessels do not , leading to an imbalance of blood flow favoring the normal vessels causing a “defect” in atherosclerotic vessels’ distribution. ADENOSINE STRESS •Contraindicated in bronchospasmic patients: Most COPD are not bronchospasmic. Ask if patient was ever intubated, prednisone dependent or nebulizer dependent. 1. Rx stop infusion 2. Rx Theophylline •Contraindicated in high gradient AV block: If block down Rx, stop infusion, Rx atropine. •If patient is on Theophylline or Dyperidamole chronically, hold drug for 24 hours. •Caffeine extinquishes the effects of Adenosine and you do not really have a stress test. ADENOSINE THALLIUM IS ESPECIALLY GOOD IN PATIENTS 1. LBBB – native or PACEMAKER induced: Stress and Dobutamine – both from the inability to interpret septal wall defects due to LBBB. There is not as much variation in motion of septum in adenosine stress. 2. Pre-op AAA NUCLEAR IMAGING • Thallium – Thallium • Thallium – Sestamibi exercise • Sestamibi – Sestamibi for very obese patients – 2 days, more Sestamibi on stress day • Adenosine – walk test – save one hour of wait time to image stress and avoid bradycardia and symptoms (Short) Apex (Vertical) Sept (Horizontal) Inf Berman, DS ; 1st Virtual Congress of Cardiology DOBUTAMINE protocol for echo or nuclear imaging • Catecholamine – Increases HR and BP, but also vasodilates so BP drop. • Start at 5 mcg/kg/min if looking for viability but usually 10, 20, 30, 40, 50 mcg/kg/min for 3 minutes infusions (begin imaging at 2 minutes) • Use Atropine in .25 mg increments – start at 30 mcg/kg/min if HR is less than 100 there. Cautions in Dobutamine • Caution in: – Rapid Afib, VT – use metoprolol 5 mg IV I mg/min push – Hypertension – dobutamine can raise or lower blood pressure - may need to stop if you are starting out high. Can use atropine to get to goal if note BP is going to be limiting. – Migrainers can get severe vasodilatory headaches – Schizophrenic or other mentally unstable patients may not tolerate the catecholamine effects of dobutamine – test may need to be aborted. DOBUTAMINE STRESS ECHO Dobutamine stress echo is especially good for • Asthmatics • Obese patients – can dodge the anterior wall attenuation artifact of nuclear imaging 16 SEGMENT MODEL Diagram of the modified 16-segment model with areas of coronary artery distribution shown as areas of stippling or cross hatching. The overlap areas are represented as a combination of the graphics in the overlap territory. ANT = anterior; 4C = four chamber; INF = inferior; LAT = lateral; LAX = long axis; POST = posterior; SAX PM = short axis at the papillary muscle level; SEPT = septal; 2C = 2 chamber. Segar DS et al. JACC 1992; 19:1199 WALL MOTION SCORE Give each segment a score. Normal – 1 Hypokinetic – 2 Akinetic – 3 Dyskinetic – 4 Aneurysmal – 5 Add up all segment scores and divide by number of segment seen. 1 is normal. ******* WMS 2.5 or greater is a poor prognosis. A 16-segment model can be used, without the apical cap, as described in an ASE 1989 document. A 17-segment model, including the apical cap, has been suggested by the American Heart Association Writing Group on Myocardial Segmentation and Registration for Cardiac Imaging. Will be most useful if and when echo perfusion imaging is available. Lang et al. J Am Soc Echocardiogr 2005;18:1440-1463 Typical distributions of the right coronary artery (RCA), the left anterior descending (LAD), and the circumflex (CX) coronary arteries. The arterial distribution varies between patients. Some segments have variable coronary perfusion. Lang et al. J Am Soc Echocardiogr 2005;18:1440-1463 Caveats in Stress echo • False positives are seen in patients with hypertensive responses to exercise and in patients with cardiomyopathies. The LBBB does not disqualify a patient from a stress echo as you CAN read the anterior wall looking for an LAD lesion. The septal and anteroseptal walls are influenced by the LBBB so can not be used. Sensitivity Specificity • ECG alone 53% vs 83% • Spect 90% vs 80% • Echo 85% (*80% single vx) vs 85%