Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
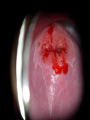
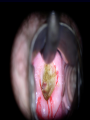
Gynaecological Cancers Malcolm Padwick MD FRCOG Cervical Cancer Cervical Cancer • • • • 1992 national targets set for year 2000 1. Reduce mortality by 20% 2. Achieve 80% smear uptake 1991 targets had already been achieved Mortality rate had been falling since 1950 at a rate of 1 -2 % per annum Now 2.3 per 100000 At risk groups Young (immature TZ) Early age of first sexual intercourse Multiple partners Smoking Type of contraception Screening history Screening intervals (2004) Age Group (years) 25 Frequency of Screening First invitation 25 - 49 3 yearly 50 - 64 5 yearly 65+ No screen since age 50 yrs or recent abnormal smear HPV 1. 2. 3. HPV subtyping will become available Concentrate screening on genuinely at risk women Allow an increase in the screening interval Avoid unnecessary intervention Referral to Colposcopy 3 inadequate smears 2 mildly dyskariotic / borderline smears First moderately or severely dyskariotic smear Glandular abnormalities Suspicion of malignancy Colposcopy visit Information sheets with appointment Separate clinic waiting area Changing and washing facilities Separate consultation area Comply with NHSCSP appointment waiting times Comply with NHSCSP waiting times for results Scale of problem Watford referrals 1995 Watford referrals 2003 228 new patients 618 new patients Therefore a follow-up policy change introduced (NHS) Colposcopy 1. 2. Assess Biopsy and act on results when available See and treat After effects 3 weeks of diminishing blood stained discharge Risk of secondary infection at 1 week Next period often heavy and painful Overall post operative pain is minimal >98% have a clear or better smear result at 6 months Cervical cancer From colposcopy General clinic with abnormal bleeding Acute admission with symptoms of advanced disease Staging EUA and cystoscopy Pelvic MRI Abdominal and chest CT Normal uterine anatomy Pre-menopausal Post-menopausal Stage IIIB - pelvic sidewall or ureteric obstruction MRI signs: n Same findings as IIB with involvement of obturator, piriformis , levators muscles n Hydroureter Treatment 1. 2. 3. 4. 5. Surgery Cone biopsy Radical trachylectomy Radical hysterectomy Neoadjuvant chemotherapy combined with radical surgery exenteration Treatment Chemo-radiation as a primary treatment Radiotherapy as post operative treatment for poor prognostic disease Chemotherapy or radiotherapy for palliation consequences 1. 2. 3. 4. Surgery Acute complications Fistula Bladder dysfunction Body image General improvement with time. consequences 1. 2. 3. 4. 5. Chemoradiation Alopecia Radiation burns Vaginal stenosis and inflammation Cystitis and colitis Fistula bowel and bladder Side effects tend to get worse with time. The future Improved prevention Less invasive treatment for pre-cancer vaccination outcome Stage 5 year survival I II III IV 80% 60% 20% 5% Malcolm Padwick MD FRCOG Gynaecologist West Herts NHS Trust Ovarian Cancer General impression Middle class disease Effects older population Silent killer One of the diseases GPs fear missing the most Mortality 12 per 100000 At risk groups Post menopausal Nulliparous Family history (including breast cancer) Contraceptive usage Endometriosis Environmental Screening • Genetic - BRCA 1 and 2 mutations USS and CA125 ????? Prophylactic oopherectomy after 40 years +/- HRT • General population USS and CA125 ????? Research projects only presentation Abdominal distension Abnormal PV bleeding Abdominal discomfort Dyspepsia Bowel symptoms From physicians and general surgeons Investigations CA125 USS laparoscopy CT MRI Typical peritoneal nodules of ovarian cancer Management MDT Surgery +/- chemotherapy Staging and randomization into interval debulking study Interval debulking Pregnancy associated mass Peritoneal nodules of ovarian cancer before and after carboplatin Follow-up CA125 CT Relapse chemotherapy Relapse surgery Outcome Stage 5 Year survival I II III IV 90% 70% 25% 5% Future ? Endometrial Cancer Malcolm Padwick Endometrial Cancer 65 of all cancers in women postmenopausal obese (hypertensive, diabetic) HRT tamoxifen Symptoms PMB IMB PCB Pap smear Pain Weight loss, bowel and bladder changes Abnormal bleeding on HRT Managment Refer to the “rapid access clinic” Use cancer pro forma Investigations Pelvic USS If endometrial signal > 4mm for endometrial biopsy -- either pippelle or hysteroscopy and currettage High risk symptoms go straight to H & C