Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
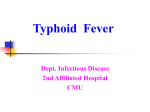
Typhoid fever You Chengcheng Dept. of pathology China Three Gorges University 1 Contents Introduction Pathogenesis Pathological changes Symptoms Complication 2 First, let me tell a story of typhoid Mary …… 3 Prevalent in the third world country Outbreaks are rare,but in some areas such as in Indonesia and New Guinea,it ranks among the 5 most common causes of death Bacterial infection of the intestinal tract and occasionally the bloodstream The ileum is most affected 4 Mononuclear Phagocytic System(MPS): Monocytes and its derivations mononuclear cells (blood) macrophages (connective tissue) kupffer cells (liver) ……….. Typhoid fever is characterized by macrophages Proliferation of MPS, which are particularly predominant in ileum. 5 Pathogenesis The germ that causes typhoid is a unique human strain of salmonella called Salmonella typhi Gram negative bacillus. O-Ag, H-Ag, vi-Ag (Widal reaction) 6 Infection source:typhoid fever patient and carrier route of transmission: fecal-oral route susceptible population:children and young people Food, fly, finger, water 7 second contact First contact Salmonella typhi Contaminanted food Proliferate in ileum tissue bacteremia Whole body Lymph tissue Septicaemia in ileum Toxemia Gall bladder Excretion Incubation period(10 d) Hyperplasia stage (1w) Necrosis and ulceration (2w) Healing (1w) 8 9 Pathological changes Hallmark histologic finding:the infiltration of tissue by typhoid cells typhoid cells:large macrophages contain Phagocytized erythrocytes, lymphocytes, bacteria and necrotic cellular debris Typhoid nodule (typhoid granuloma) : the aggregates of typhoid cells 10 Typhoid nodule can present in the lymph tissue of small intestine, mesenteric lymph node, the liver, spleen and marrow, its typical changes often occur in the lower part of ileum , especially in the Peyer‘s patches and Isolated lymphonodulus. 11 typhoid cell 12 typhoid cell 13 typhoid cell 14 typhoid cell 15 Typhoid granuloma 16 Intestinal pathological changes The principal lesions are those of lymphoid tissue of terminal small intestine. (1) Hyperplasia Stage ( Peyer’s patches) (2) Necrosis Stage; (3) Ulceration Stage; (4) Healing Stage. 17 Hyperplasia stage: the 1st w after onset lymphoid tissue swelling protrude out the mucosa , looks like cerebral convolution 18 Hyperplasia stage Showing the hyperplasia of Peyer’s patches of ileum, which is button-like elevation 19 Hyperplasia stage looks like cerebral convolution 20 Hyperplasia stage looks like cerebral convolution 21 Hyperplasia stage 22 Microscopy: 23 24 •Necrosis stage: the 2nd w after onset multi-focal necrosis in lymphoid tissue 25 Ulceration stage: the 3rd w after onset, necrosis tissue fall off and ulcer formation, longitudinal ulcer is parallel with the axis of intestinal canal , deep to the muscularis layer and involve the artery ,which will result in bleeding 26 ulceration stage Key features: • Round or oval •Elevated margins •Uneven bottom •Parallel to the axis of intestine 27 ulceration stage Key features: • Round or oval •Elevated margins •Uneven bottom •Parallel to the axis of intestine 28 ulceration stage ulcer 29 Difference Typhoid fever Tuberculosis 30 Healing stage: the 4th w after onset Granulation tissue proliferation , scar formation 31 Changes in other MPS Typhoid nodule formation and ulceration in mesenteric lymph node, the liver, spleen and marrow. 32 Lesions in other organ Gall bladder: carrier Heart: slower pulse Kidney: Albuminuria Skin: rose rashes 33 SYMPTOMS Fever (some as high as 40 Degrees) Weakness Headache Loss of Appetite Stomach pains Rose Rashes 34 35 Complications: intestinal bleeding intestinal perforation lobular pneumonia 36 37 Bacillary Dysentery Chengcheng You Dept. of pathology China Three Gorges University 38 Bacillary dysentery is an acute bacterial infection caused by the genus Shigella resulting in colitis affecting predominantly the rectosigmoid colon. The disease is characterized by diarrhea, dysentery, fever, abdominal pain, and tenesmus. It is usually limited to a few days. Mainly occur in infants and young children 39 •Pathogen Shigellae are nonmotile gram-negative bacilli belonging to the family Enterobacteriaceae •Four species: S. dysenteriae (group A), S. flexneri (group B), S. boydii (group C), S. sonnei (group D). 40 Incidence •most cases of shigellosis occur in children of developing countries •S. flexneri is the predominant species •Children between 1 and 4 years old 41 • Infection source: patient and carrier • route of transmission: fecal-oral route • Susceptible population:children and young people • seasonal patterns: autumn and summer 42 PATHOGENESIS •organisms traverse the small bowel, penetrate colonic epithelial cells and multiply intracellularly •acute inflammatory response •pseudomembranous type of colitis •Epithelial cells containing bacteria are lysed, resulting in superficial ulcerations and shedding of shigella organisms into stools •Diarrhea results because of impaired absorption of water and electrolytes by the inflamed colon 43 Feature Location: predominantly the rectosigmoid colon Clinical type : Acute bacillary dysentery Chronic bacillary dysentery Toxic bacillary dysentery 44 Acute bacillary dysentery Serous inflammation Mucus secretion increase diffuse hyperemia erosion Fibrinous inflammation Map-like ulcer bloody mucoid diarrhea healing 45 Acute bacillary dysentery •Gross: Affect the colon, producing an acute inflammation with diffuse hyperemia、 edema and multiple superficial ulcers. •Pseudomembrane formation: exudate fibrin, neutrophils, necrotic debris, bacteria •MI: epithelial cell necrosis, fibrin exudation monocytes and neutrophils infiltration abscess formation •The lesions are often self-limited and can recover completely 46 Pseudomembrane 47 pseudomembranous inflammation Gross: showing the pseudomembrane and irregular ulcers 48 bacillary dysentery 49 50 Microscopy: 51 Bacillary dysentery 52 53 Complications •Intestinal Bleeding •Intestinal Perforation(seldom) 54 Clinic Feature Symptoms begin with sudden onset of high grade fever, abdominal cramps and watery diarrhoea. Subsequently diarrhea become mucoid, of small volume and mixed with blood. This is accompanied by abdominal pain and tenesmus. Physical signs are those of dehydration beside fever, lower abdominal tenderness and normal or increased bowel sounds. 55 Chronic bacillary dysentery •lasting more than 2 months , infected by S.flexneri(福氏菌). •Clinical features: Mild symptom of abdominal pain ,diarrhea Infectious source •pathological changes: ① chronic ulcers; ② forming polypi ; ③ intestinal wall are fibrosis. 56 Toxic bacillary dysentery Children at the age of 2-7 years old are sensible most are result from S.sonnei and S.flexneri. clinical features: ① toxic symptom all over the body: Toxic shock、respiratory or circulation failure. ② intestinal symptom: mild 57 Questions for the class 1.What kind of inflammation is involved in bacillary dysentery? 2.The definition of typhoid granuloma 58