Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Bacterial cell structure wikipedia , lookup
Horizontal gene transfer wikipedia , lookup
Gastroenteritis wikipedia , lookup
Infection control wikipedia , lookup
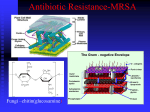
Methicillin-resistant Staphylococcus aureus wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Anaerobic infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Triclocarban wikipedia , lookup
Urinary tract infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
ANTIMICROBIAL AGENTS AND PRINCIPLES OF THERAPY Prof T Rogers Clinical Microbiology TCD SOME GENERAL PRINCIPLES • Antibiotics can be naturally produced, semi-synthetic, or synthetic substances • Designed to have as much selective toxicity on the bacteria as possible • This is more likely to be achieved compared to antimicrobials acting against eukaryotic cells (fungi, protozoa) EXAMPLES OF SELECTIVE ACTION • Penicillin on bacterial cell wall (organisms without cell wall won’t be inhibited eg Mycoplasma pneumoniae) • Sulphonamides prevent bacteria synthesising folic acid whereas humans can use preformed folate • Generally drugs acting on cell membranes or protein synthesis are more toxic to humans The Penicillin Molecule ANTIBIOTICS ACTING ON CELL WALL OF BACTERIA • BETA LACTAMS: • Penicillins, cephalosporins, carbapenems, • GLYCOPEPTIDES: • Vancomycin, teicoplanin THE IDEAL ANTIBIOTIC?:PENICILLIN • • • • • • • Narrow spectrum Bactericidal Very selective mode of action Doesn’t disturb gut flora Low serum protein binding Widely distributed in body esp. CNS Excreted by the kidneys BENZYLPENICILLIN: MAIN INDICATIONS Strep pyogenes sepsis (from sore throat to fasciitis) Pneumococcal pneumonia, meningitis Meningococcal meningitis, sepsis Infective endocarditis (strep) Strep group B sepsis Diphtheria Syphilis, leptospirosis THE DEVELOPMENT OF THE BETA LACTAMS • Benzylpenicillin and early cephalosporins mainly active against gram positive bacteria (strep and staph) • Cloxacillin: stable to penicillinase • Then “broad spectrum” penicillins appeared: ampicillin, ureidopenicillins and cephalosporins: cefuroxime, cefotaxime • Carbapenems and latest generation of cephalosporins, eg ceftazidime more active against gram negatives • Monobactam: aztreonam CLOXACILLIN (METICILLIN) • • • • • Narrow spectrum: Staph aureus (MSSA) Stable to TEM1 beta lactamase Similar antibiotics are meticillin, nafcillin Similar safety profile to benzylpenicillin MRSA emerged in the early 1970’s (MecA gene encoding additional pbp) BROADER SPECTRUM PENICILLINS • Ampicillin, amoxycillin cover most organisms hit by penicillin but also Esch coli, some Proteus (cause UTI’s) • Augmentin stable to TEM1 beta lactamase because of the clavulanic acid therefore more active than ampicillin • Tazocin: broader coverage than augmentin against gram negatives including Pseudomonas PENICILLIN IS GENERALLY VERY SAFE BUT…. • Allergic reactions not uncommon-rashes • Most severe reaction being anaphylaxis • A history of anaphylaxis, urticaria, or rash immediately after penicillin indicates risk of immediate hypersensitivity after a further dose of any penicillin or cephalosporin (therefore these must be avoided) • Allergy is not dependent on the dose given ie, a small dose could cause anaphylaxis • Very high doses of penicillin can cause neurotoxicity • Never give penicillin intrathecally What antibiotics can be used in penicillin allergy? • Macrolides: erythromycin, clarithromycin • (mainly gram positive cover) • Quinolones: ciprofloxacin, levofloxacin (mainly gram positive cover) • Glycopeptides (serious infections) • Fusidic acid, rifampicin, clindamycin (mainly gram positive) REMEMBER WHAT THE OTHER BETA LACTAMS ARE: • All penicillins: ampicillin, augmentin, piperacillin, cloxacillin • Cephalosporins: cefuroxime, cefotaxime, ceftriaxone, ceftazidime (5-10% cross sensitivity) • Monobactam: aztreonam (low cross sensitivity) • Carbapenems: imipenem, meropenem CEPHALOSPORINS: MAIN USES • Cefuroxime: surgical prophylaxis • Cefotaxime/ceftriaxone: meningitis nosocomial infections excluding Pseudomonal, • Ceftazidime: nosocomial infections including those caused by Pseudomonas Problems with antibiotic resistance: how does it happen? • Some bacteria are naturally resistant to particular antibiotics (Pseudomonas has permeability barrier to many antibiotics) • Some typically susceptible species have minority populations which are resistant by virtue of mutational resistance (pneumococcus) • Other species acquire resistance via plasmids (“infectious resistance”) eg Neisseria gonorrhoeae, many gram negatives PENICILLIN RESISTANCE: Organisms producing TEM1beta lactamase • • • • • Haemophilus influenzae Neisseria gonorrhoeae Bacteroides fragilis Staph aureus Esch coli What are ESBL’s??? • Enzymes which have a broad spectrum of activity against third generation cephalosporins eg cefotaxime • Can be carried on extrachromosomal plasmids which additionally encode resistance to eg, fluoroquinolones, aminoglycosides • Can be spread between different enterobacteria by conjugation • As big a threat as MRSA CARBAPENEMS • Imipenem, meropenem: have a very broad spectrum activity against gram-negative bacteria, anaerobes, streps • Now used to treat gram negative infections due to so called ESBL producing organisms eg, E coli, Klebsiella • Ertapenem is a new member of the group but its not active against Pseudomonas A new threat posed by antibiotic resistance: NDM-1 • Confer resistance to carbapenems which are among our most efffective antibiotics • Pose a new threat • Often linked to travel to India but now reported around the World Community Healthcare ass’d Hospital More resistance Less resistance Current major antibiotic resistance problems: community infections • Respiratory tract: penicillin resistance in pneumococcus (5-10%) • Gastrointestinal: quinolone resistance in Campylobacter • Sexually transmitted: penicillin, quinolone resistance in gonococcus • Urinary tract: beta lactam resistance in Esch coli • Tropical: multidrug resistance in Salmonella typhi, Shigella spp Current major resistance problems: hospital infections • MRSA: current strains are often multiplyantibiotic resistant • VISA/GISA: intermediate resistance to glycopeptides (thickened cell wall) • VRSA/GRSA: highly resistant (transferable on plasmids) from enterococci • VRE: enterococci (multiply resistant) • Broad spectrum beta lactam resistant (ESBL) and quinolone resistant Esch coli, Klebsiella • Multiply antibiotic resistant enterobacteria: Acinetobacter, Stenotrophomonas, Serratia © July Issue of Epi-Insight, Vol 6, Issue 7, Health Protection Surveillance Centre, Ireland S. aureus BSI 2006 HOSPITAL HA ACQ’D Antibiotic name Erythromycin Oxacillin Cloxacillin Linezolid Vancomycin Number 78 78 78 78 %R 56.4 65.4 0 0 HCA Number %R 24 54.2 24 50 24 0 24 0 COMMUNITY NHCA Number 18 18 18 18 %R 33.3 27.8 0 0 M R S A E. coli - distribution of fluoroquinolone (CIP/OFX) resistance in EARSS countries in 2005 EARSS in Ireland – E. coli trends 1800 21 27 40 42 42 25% 1600 Number of isolates 1200 15% 1000 800 10% 600 400 5% 200 0 0% 2002 2003 2004 2005 2006 Time period Total E.coli %3GC-R %CIP/OFX-R Changes in the numbers of participating laboratories are indicated above the bars %GEN-R % Resistance 20% 1400 TUBERCULOSIS The Threat of Multi-Drug Resistant (MDR) T.B. o HIV patients o Erratic or incomplete treatment o Non-compliance o Persistent symptoms despite treatment o Resident in area of high prevalence eg, Former Soviet countries Other major antibiotic groups: aminoglycosides • Gentamicin, amikacin (tobramycin, streptomycin) • Mainly active against gram negative bacteria • Mainly used to treat nosocomial infections: pneumonia in ITU, septicaemia • Limiting factors are nephrotoxicity (and ototoxicity) and resistance • Also used in combination How we give aminoglycosides • For serious nosocomial infections: “extended interval” or once daily dosing • 5 or 7mg/kg/day for gentamicin (Hartford nomogram) • Rationale based on concentrationdependent killing and post-antibiotic effect • Reduced risk of nephrotoxicity • In infective endocarditis use lower doses to give synergy with penicillin Some other antibiotics occasionally used • Co-trimoxazole (Stenotrophomonas) • Chloramphenicol (typhoid fever, meningitis) • Colistin (resistant Pseudomonas) topical • Neomycin: gut decontamination, topical Some indications and limitations of particular antibiotics COMMUNITY ACQUIRED PNEUMONIA: WHAT’S CAUSING IT? TYPICAL GRAM APPEARANCE OF Strep pneumoniae IN SPUTUM GRAM POSITIVE CHAINS DIPLOCOCCI Community acquired pneumonia • Pneumococcus (and H influenzae) are most likely: therefore ampicillin, amoxycillin or augmentin • Severe pneumonia: cefotaxime • Severe atypical pneumonia (Legionella): macrolide or quinolone • Resistant pneumococcus: vancomycin or linezolid (new antibiotic!) • A new quinolone moxifloxacin covers most of these pathogens (likely to be used more in community) S. pneumoniae Antibiotic name Cefotaxime Erythromycin Penicillin G *MIC 0.12 -1.0 mg/l **MIC >= 2mg/l Num. 60 222 221 %R 0 17.6 2.7** %I 16.7 1.4 22.2* %S 83.3 81.1 75.1 Lower Respiratory Tract Infection Antibiotic Guidelines Infection Common Pathogens Recommended antibiotics (i) Community Acquired Pneumonia S. pneumoniae, H. influenzae, Mycoplasma, Legionella Co-amoxiclav ,Clarithromycin (ii) Exacerbation of Chronic Obstructive Pulmonary Disease S. pneumoniae, H. influenzae Moraxella sp. Co-amoxiclav , Moxifloxacin (iii) During influenza epidemic Consider S. aureus Fluclox, Vancomycin (iv) Hospital/institutional acquired pneumonia Aerobic Gram-negatives Legionella, S. aureus PipTaz, Cipro gentamicin (v) Aspiration pneumonia a) Community Acquired Aerobic & anaerobic strep b) Nosocomial Aerobic Gram-negatives Community acquired urinary tract infections • • • • • • • Ampicillin, amoxycillin, augmentin Oral cephalosporin: cephradine Trimethroprim Nalidixic acid Nitrofurantoin Ciprofloxacin Mecillinam Top Five URINARY isolates SJH 2006 HA n = 1432 E. coli HCA n = 562 605(42%) E. coli NHCA n = 870 306(54%) E. coli 608(70%) Enterococcus sp 230(16%) Enterococcus sp 87(16%) Enterococcus sp 67(8%) Klebsiella sp. Klebsiella sp. 50(9%) Klebsiella sp. 40(5%) P. mirabilis 30(5%) P. mirabilis 28(3%) P. aeruginosa 14(3%) Coag neg Staph 25(3%) P. mirabilis S. aureus 162(11.3%) 100(7%) 31(2%) One isolate per patient included E. coli from Urine HA Antibiotic name Number Amoxicillin/Clavulanic 604 acid Ampicillin 603 Ciprofloxacin 603 Gentamicin 278 Meropenem 277 Nitrofurantoin 604 Piperacillin/Tazobactam 278 Trimethoprim 604 %R 13.1 68 33.3 16.2 0 4.5 5 45 HCA Number 303 303 305 114 115 305 115 303 %R 7.9 63 24.3 14 0 2.3 0.9 39.3 NHCA Number %R 606 3.8 604 55.5 606 7.3 85 7.1 85 0 605 2.8 85 3.5 605 34.2 Genitourinary infections Antibiotic Guidelines Infection Urinary Tract Infection 1. simple cystitis: non- catheter related, non-pregnant women, no prior treatment in community Common Pathogens E. coli Other Gram-negative rods Less commonly: Enterococci Staph. saprophyticus 2. recent treatment or hospitalised Recommended antibiotics Trimethoprim Nitrofurantoin Ciprofloxacin Ciprofloxacin 3. Catheter-related Pyelonephritis or Complicated UTI E. coli Ciprofloxacin Co-amoxiclav Ceftriaxone IV Gentamicin HA Cipro Resistant E.coli 410 patients with HA Cipro resistant E. coli from 2003 – 2006 29% were Care of the Elderly patients (speciality) 62% were from urine with and w/o catheter Cipro resistance and usage 30 12000 25 10000 20 8000 15 6000 10 4000 5 2000 0 0 Q3 Q4 2003 Q1 Q2 Q3 2004 Q4 Q1 Q2 Q3 2005 Q4 Q1 Q2 2006 DDD ciprofloxacin in SJH % resistance of E. coli to ciprofloxacin Ciprofloxacin Resistance in E. coli Skin and soft tissue infections • Cellulitis ? Streptococcal: penicillin or augmentin • Infected eczema ? Staphylococccal/mixed: penicillin+flucloxacillin or augmentin • Necrotising fasciitis: penicillin+clindamycin • Septic arthritis: fluclox+fusidic acid • Gangrene: metronidazole Where there is deep-seated infection: bone, abscess • Need an antibiotic with good tissue and phagocyte penetration • Examples are rifampicin, clindamycin, fusidic acid, ciprofloxacin, metronidazole • So for treatment of Staph aureus osteomyelitis: flucloxacillin+ fusidic acid Why do we use combination therapy? • When treating serious infection empirically we want to cover a broad spectrum (severe pneumonia:cefotaxime+erythromycin) • To prevent the emergence of drug resistance: tuberculosis regimens • For synergy: infective endocarditis (aminoglycoside) • For mixed infections eg, abdominal sepsis (tazocin+metronidazole) Are we moving to the Postantibiotic era? o Judicious use of current antibiotics both in Hospital and Community o New antibiotics o Improve Infection control practice o Better management of hospitalised patients New antibiotics • Daptomycin: lipopeptide active against strains of Staph aureus (incl MRSA) and VRE (bactericidal) • Mode of action: disrupts bacterial cell membrane • Given intravenously • Indicated for skin and soft tissue infections and R sided endocarditis, bacteraemia due to S aureus • Can cause myopathy (monitor CPK weekly) Tigecycline • A new glycylcycline antibiotic of tetracycline class • Broad spectrum of activity • Mode of action: bact. ribosomal synthesis • Indicated for skin and soft tissue, and intraabdominal infections • Has activity against MRSA, VRE, ESBL producing enterobacteria • Monitor liver function Linezolid • • • • An oxazolidinone antibiotic Inhibit bacterial protein synthesis Bacteristatic Active against gram positive bacteria incl MRSA and VRE • Can be used in pneumonia, skin and soft tissue infections • Thrombocytopenia and interactions with SSRI’s 9serotonin release http://www.ndsc.ie/A-Z/MicrobiologyAntimicrobialResistance/EuropeanSurveillanceofAntimicrobialConsumptionESAC/ Self assessment: Which one of the following is often resistant to penicillin because of TEM1 encoded penicillinase production: • • • • • Streptococcus pneumoniae Neisseria meningitidis Streptococcus pyogenes Mycobacterium tuberculosis Neisseria gonorrhoeae Self assessment: which one of the following is not available for oral administration in a case of systemic infection • • • • • Augmentin Ciprofloxacin Gentamicin Erythromycin Rifampicin Self assessment:Which of the following is a beta lactam antibiotic • • • • • Clarithromycin Augmentin Nitrofurantoin Nalidixic acid Fusidic acid Self assessment:In a patient with a history of anaphylaxis when previously given penicillin which one of the following should be a safe alternative • • • • • Clarithromycin Cefuroxime Augmentin Flucloxacillin meropenem