Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
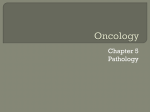
LUNG CANCER Jennie Hocking, MPAS, PA-C FIGURE 1 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths, by Sex, United States, 2008 From Jemal, A. et al. CA Cancer J Clin 2008;58:71-96. Copyright ©2008 American Cancer Society EPIDEMIOLOGY Men: Rates declining Women Rates still increasing More likely to be nonsmokers United States Cancer Statistics, 2001: Incidence and Mortality EPIDEMIOLOGY-TEXAS www.cdc.gov/cancer/lung/statistics/race.htm ETIOLOGY-GENETICS Polyfactorial Inactivated tumor supressor genes Tumor promotors Stem Epidermal growth factor receptor (EGFR) Vascular endothelial growth factor (VEGF) cells Chest. 2006;130:936-937 ETIOLOGY-GENETICS Family First reports >40 years ago Approx 2-fold increase risk for lung cancer History/Clustering Corrected for tobacco usage 10-15% of lung cancer patients have at least one affected 1st-degree relative No single gene isolated ETIOLOGY Tobacco Cigars & pipes Secondhand smoke Cigarettes directly alter mucosal barriers Chronic inflammation Ciliary dysfunction SMOKING HISTORY 46 million US smokers (23% of population) 1 pack per day x 40 years = 40 pack years OR 2 packs per day x 20 years = 40 pack years Greatest risk for lung cancer: >30 pk yrs 20 year lag period Risk declines with tobacco cessation 15 year window SMOKING HISTORY Cigarettes/pack = 20 Marlboro Math 146,000 cigarettes 1 ppd x 20 years = Retirement Savings: 2ppd x 50 years Assume 10% annual interest Retirement savings lost: $2,598,693 ETIOLOGY Other Causes Asbestos Radon Silica COPD Idiopathic PATHOLOGY Two main categories: Small Cell (20%) Non-small Cell (NSCLC) Large cell (9%) Adenocarcinoma (and bronchoalveolar) (32%) Squamous (30%) “Others” Carcinoid, sarcomas, mucoepidermoid carcinomas and undifferentiated, mesothelioma PATHOLOGY Small cell (oat cell) Extremely rapid growth Central location http://radiology.rsnajnls.org/content/vol236/issue3/images/s mall/r05se22g03b.gif PATHOLOGY Squamous cell Central location Exfoliates Aggressive imaging.consult.com PATHOLOGY Adenocarcinoma Slow growing Peripheral location “Scar” tumor More common in nonsmokers PATHOLOGY Bronchoalveolar (BAC) Form of adenoca Nonsmokers Mucous producing Peripheral ‘Ground glass’ www.argjiro.net/albi/white/path/?album=148photo.id=49 PATHOLOGY Large cell Poorly differentiated Peripheral Rapid growth CLINICAL PRESENTATION 2-15% asymptomatic Symptoms related to: Local Tumor Growth Local Spread of Tumor Metastasis Paraneoplastic Syndromes LOCAL TUMOR GROWTH Cough: pleura irritation of endobronchial mucosa or Dyspnea: obstruction, post-obstructive pneumonitis Hemoptysis: Wheezing: +/- minimal or massive endobronchial obstruction consolidation on exam LOCAL SPREAD OF TUMOR Chest pain: chest wall invasion Hoarseness: left recurrent laryngeal nerve Effusion Axillary/supraclavicular lymphadenopathy SVC syndrome: right paratracheal node or RUL tumor compression www.meddean.luc.edu/.../lungca.svcphy.html LOCAL SPREAD Pancoast OF TUMOR Syndrome Superior sulcus tumor Compresses brachial & cervical nerve roots Manifestations: Horner’s syndrome Anhydrosis Arm pain/atrophy www.mrcophth.com/.../oculoplasticgallery.html DISTANT METASTASES Contralateral lung Liver Elevated LFTs Adrenals Bone Elevated Calcium Bone pain Pathologic fractures Brain ±Neurologic signs/symptoms PARANEOPLASTIC SYNDROMES Endocrine hormone secretion PTH-like hormone secretion SIADH ACTH Clubbing Anorexia, weight loss/cachexia, fever Other syndromes Lambert-Eaton Syndrome Hypertrophic pulmonary osteoarthopathy Hematological abnormalities DIAGNOSIS & STAGING Goal #1 Obtain a tissue diagnosis and determine the stage of malignancy efficiently and safely Goal#2 Determine patient candidacy for therapy CHEST XRAY (CXR) Relatively low cost Readily available Insensitive Difficult to see all regions of chest Non-specific if no symptoms <5% of solitary pulmonary nodules in mass screening Screening NOT proven to impact mortality Evaluate further w/CT scan US Preventive Services Task Force, 2004 CHEST CT More sensitive Size, shape, and invasion Evaluate lymphadenopathy Pitfalls: Radiation exposure Cost Moderate specificity Not recommended for screening CHEST CT Approach: Establish chronicity Incidental, asymptomatic, <1cm, benign appearance, low risk patient Symptomatic, risk factors, >1cm or growing on serial scans Definitive workup DIAGNOSIS-PET Radiolabeled glucose Metabolically active cells Uses Heart, brain, kidneys, bladder Cancer, infection Determine activity of known masses Locate distant metastasis Pitfalls Can miss slow growing tumors Can’t differentiate between tumor/infection Doesn’t accurately measure size, growth DIAGNOSIS-TISSUE Sputum Cytology Least invasive Tumor location important Not recommended for screening DIAGNOSIS-TISSUE Bronchoscopy Central lesions Endobronchial tumors Fluoroscopic guidance for peripheral tumors Mediastinal biopsies DIAGNOSIS-TISSUE Needle Biopsy Good specificity Sensitivity varies Operator dependent Pneumothorax DIAGNOSIS-TISSUE Surgical Lung Biopsy Thoracotomy is gold standard Increased use of VATS CME for staging/dx DIAGNOSIS-OTHER Labs: STAGING STUDIES CBC, chemistry panel w/calcium, coag panel, LFTs MRI of brain CT abdomen/pelvis Biopsy of other sites ±bone scan, PFTs w/ABGs echo, V/Q scan TREATMENT Smoking cessation Nutrition Surgery Chemotherapy Radiation Other Palliative Care Airway stents/laser Indwelling pleural catheters Pain control Hospice +/- Emotional support http://www.co.jackson.mi.us/HD/images/PrevNews/GreatAmericanSO.jpg STAGING-NSCLC TNM system T-tumor size &/or location N-lymph nodes M-metastasis Stage I (T1aN0M0)-Stage IV (TanyNanyM1or2) STAGING, TREATMENT & PROGNOSIS - NSCLC Stage I disease No lymph node involvement Surgical removal Follow Up with CT scans 43-64% 5-year survival (surgical) Stage II & III disease Lymph nodes involved or larger tumor or multiple lung tumors Surgery, radiation & chemotherapy may all play a role in treatment STAGING, TREATMENT & PROGNOSIS- NSCLC Inoperable patients XRT (via stereotactic approach) and chemotherapy 5-25% long term survival Stage IV disease Chemo +/- XRT XRT/gamma knife for brain mets Occasionally some mets surgically resected Increases mean survival from 4-6 mo to 7-9 mo STAGING & PROGNOSIS - SCLC Limited: confined to hemithorax, regional nodes Extensive: all others (70% at diagnosis) Death in weeks to months if untreated Median survival: Limited 16 – 24 months 10-20% alive at 2 years Extensive 9 – 12 months 30% die of local tumor complications 70% die of carcinomatosis THERAPEUTICS - SCLC Highly sensitive to chemo and XRT Combination chemotherapy regimens best Surgery not useful ADDITIONAL REFERENCES Minna JD, Schiller JH. Neoplasms of the Lung. In: Fauci, AS, Kasper, DL, Longo, DL, Braunwald, E, Hauser, SL, Jameson, JL, Loscalzo, J. Harrison’s Principles of Internal Medicine, 17th ed. New York: McGraw Hill; 2008 Detterbeck FC, Boffa DJ, Tanoue LT. The New Lung Cancer Staging System. Chest. http://chestjournal.chestpubs.org/content/136/1/260.full.pdf+html PACE curriculum, School of Allied Heath Sciences, Baylor College of Medicine, 2008 Hoopman, Todd, MD. PA lung cancer. 2006 Cedar Bluff CME. Neoplastic Disease. 2007 Humphrey L, Teutsch S, Johnson M. Lung cancer screening with sputum cytologic examination, chest radiography and computed tomography: An Update for the US Preventative Services Task Force. Ann Intern Med. 2004;140:740-753.