Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
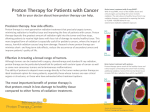
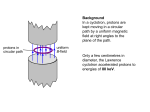
The Ultimate Healing Beam: The Future is Now John Han-Chih Chang, MD Radiation Oncologist CDH Proton Center, a ProCure Center Primary Investigator for the Radiation Therapy Oncology Group Primary Investigator for the Children’s Oncology Group Children’s Memorial Hospital Vice Chair of the Midwest Children’s Brain Tumor Clinic Road Map Background History – When and Where Proton Mechanics – How to Applications/Prostate Cancer – What for Conclusion High End Image Guided Glorified Tanning Booths Modality and Delivery Must Work Together Techniques to Improve Radiation Delivery Radiation Modality OPTIMAL RADIATION THERAPY Protons through the Ages Bragg Peak Named after the British physicist William Henry Bragg (1862 - 1942) Protons: “Ancient” History 101 Hydrogen Atom R.R. Wilson, Radiology 1946; 47:487-491 Scientists have been perfecting proton therapy as a treatment for cancer for 65 years Robert R. Wilson, PhD "Radiological Use of Fast Protons" (Radiology 1946:47:487-91) Berkeley and Harvard Fermilab Protons: History 101 1946 – Robert Wilson proposes using protons clinically 1955 – The first patient is treated at Berkley 1961 – The Harvard Cyclotron Lab (HCL) begins therapy 1991 – Loma Linda (LL) operates the first proton gantry 2001 – HCL closes NPTC opens Protons: “Modern” History 101 • • • • • • • • • Loma Linda Univ Medical Center – Loma Linda, CA 1990 MGH – NPTC Boston, Massachusetts 2002 MPRI – Bloomington, Indiana 2004 MDAH – Houston, Texas 2006 FPTI – Jacksonville, Florida 2006 PPC – Oklahoma City, Oklahoma 2009 RPTC – Philadelphia, Pennsylvania 2010 HUPTI – Hampton, VA 2010 CDH – Chicago, IL 2010 10 Proton therapy found its first clinical home in California Loma Linda First patient 1990 First facility designed as patient treatment center The CDH Proton Center, A Procure Center, Warrenville, Ill. We are dedicated to providing exceptional care in a healing environment to patients with cancer Mechanism of Action Protons have Fewer Side Effects than Photons There is no reason to irradiate healthy tissue Photons deposit only 20% of their energy in the tumor Photons deposit only 20% of their energy in the tumor Protons deposit more than 80% of their energy in the tumor Higher 20% Radiation Dose Radiation Dose Higher Prescribed Dose to Kill Tumor 80% 0% Prescribed Dose to Kill Tumor Lower Lower 70% 20% Depth in Tissue In order for photons to reach a prescribed dose at the tumor depth, healthy tissue gets four times the radiation as the tumor 10% Depth in Tissue Protons put 80% of their energy into the tumor and only 20% into healthy tissue The Physics of Protons Depth Dose Curves for Different Treatment Types High Energy X-Rays Spread Out Bragg Peak (SOBP) Relative Dose 100 80 60 40 200 MeV Protons 20 Tumor Healthy Tissue Healthy Tissue 0 0 5 10 15 20 Depth in Tissue (cm) 25 30 The Value of Protons Protons are physically superior to X-rays Protons behave differently than x-rays: Protons X-Rays do not Protons improve the “therapeutic ratio” maximizing tumor control while minimizing side effects At a given radiation dose to a tumor protons deliver, on average, less than half the radiation dose to normal tissues than do x-rays 1 16 (1) Jay Loeffler, Massachusetts General Hospital, “Proton Therapy 2009” Evidence of Distal Range Stopping Before treatment Treatment plan After treatment Why would we chose Protons? Production of Clinically-Useful Proton Beams Proton Accelerators Cyclotron (spiral path) Constant magnetic field Variable Radius Continuous Beam Treatment Delivery Production of Clinically-Useful Proton Beams Proton Accelerators - CYCLOTRON Production of Clinically-Useful Proton Beams Beam Line Energy Selection System (230 MeV 70 MeV) Beam Transport and Switching System Gantry 1 NPTC- Harvard Nozzle Snout (with aperture & compensator) 6-axis patient positioner Robotic Table Protons are delivered to patients in specialized treatment rooms Fixed Beam Room Gantry Room Clinical Indications Current Pediatrics Paraspinal Ewing’s Optic pathway glioma Optic nerve meningioma Prostate/Pelvic RMS Exophytic BSG Craniospinal irradiation Suprasellar NGGCT Prostate Head and Neck/Base of Skull Intracranial Meningioma Paraspinal/Sacrum Chordoma Planned Lung Organ motion Density changes Tumor response Inspiration: Expiration GI Organ motion Density changes Breast - API Lymphoma Ocular Prostate Cancer Radiation Treatment Options Radiation therapy options include Brachytherapy (BT) is vastly underutilized Effective Safe (in the appropriately selected patients) Convenient (1 to 2 day procedure) External Beam Radiation Therapy (EBRT): Proton beam is superior to IMRT Higher cure rates Lower complication rates Stereotactic Body Radiotherapy (SBRT) Effective Convenient (3 to 5 day non-invasive procedure) Safety seems to be similar to IMRT (it is still X-rays) Definitive Therapy Surgery Open Brachytherapy Laparoscopic (Da Vinci) Low-Dose Rate High-Dose Rate External-Beam Radiation X-Ray (IMRT & SBRT) Proton Beam Definitive Therapy Invasive Surgery Open Laparoscopic (Da Vinci) Brachytherapy Low-Dose Rate High-Dose Rate External-Beam Non-Invasive Radiation X-Ray (IMRT & SBRT) But, don’t forget about active surveillance! Proton Beam Misconceptions About Proton Therapy “Just because someone keeps saying it doesn’t make it true.” The typical quote: “The DVH of IMRT is better than the DVH of protons in the high dose region, and that’s what really counts” FACT: Protons, regardless of delivery method, and with equivalent PTVs, should yield superior DVH curves without overlap The typical quote: “There is no data showing protons have better control rates” FACT: Protons do have better control By definition, protons will never have worse control rates than x-rays Misconceptions About Proton Therapy “Just because someone keeps saying it doesn’t make it true.” The typical quote: “There is no data showing that side effects and complications (“toxicity”) are lower with protons” FACT: At a similar treatment dose and volumes, the toxicity is lower with protons The typical quote: “Protons are 2x to 5x times more expensive than IMRT” FACT: Protons are at most 40% – 60% more than IMRT, based on Medicare, and offer a much better value The lifetime costs of protons are much less than IMRT Patient access must not be based on misconceptions. We must rely on science and data to drive these decisions. Protons have Fewer Side Effects than Photons There is no reason to irradiate healthy tissue Photons deposit only 20% of their energy in the tumor Photons deposit only 20% of their energy in the tumor Protons deposit more than 80% of their energy in the tumor Higher 20% Radiation Dose Radiation Dose Higher Prescribed Dose to Kill Tumor 80% 0% Prescribed Dose to Kill Tumor Lower Lower 70% 20% Depth in Tissue In order for photons to reach a prescribed dose at the tumor depth, healthy tissue gets four times the radiation as the tumor 10% Depth in Tissue Protons put 80% of their energy into the tumor and only 20% into healthy tissue “Direct Radiation Complications Never Occur In Unirradiated Tissues” Dr. Herman Suit1 IMRT immerses more healthy tissue with radiation Radiation Therapy Plans for Prostate Cancer IMRT - 7-field co-planer Proton Therapy - 2-field DS Blue – 13% Green – 51% Purple – 63% Yellow – 76% Red – Higher dose bath to healthy tissue with IMRT: Pelvis, rectum and bladder (1) 95% Tumor Less healthy tissue exposed to radiation compared to IMRT Herman Suit, “The Grey Lecture 2001: Coming Technological Advances in Radiation Oncology,” International Journal of Radiation Oncology Biology Physics 53 No. 4 (2002): 798-809. 36 Prostate Cancer Treatment Plans Protons IMRT IMRT- Protons: Excess dose for IMRT Protons for rectum and bladder-dose is much lower Dose -% of dose IMRT immerses more healthy tissue with low to intermediate dose bath The Data: Photons vs Protons Prostate Cancer Proton Therapy vs. Conventional Radiation (by dose) in Locally Advanced Prostate Cancer Modality Dose Recurrence Complication Conventional Radiation <60 GY 38% 22% Conventional Radiation 60 – 65 GY 36% 35% Conventional Radiation 70 GY 28% 45% Conventional Radiation >75 GY 20% 60% Protons 75 GY 15% 12% Source: Presentation by Dr. N. Mendenhall, University of Florida, IBA Rectum Rectum 100 90 80 Volume The limit of the photon modality IMRT - MSK 70 3D CRT - MSK 60 IMRT - MGH 50 IMRT - UFPTI 40 Proton - MGH 30 20 Proton - UFPTI 10 0 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 Dose Adapted from Zelefsky 2000, Trofimov 2007 and Vargas 2008 Rectal dose comparison IMRT plans Rectum V70 MSKCC 14% MGH 14.5% MDACC 15.5% UF 14% Protons UF 8% Zelefsky et al Radiotherapy and Oncology 2000; 55:241-249 Trofimov et al IJROBP 2007; 69:pp. 444–453, Zhang et al IJROBP 2007; 67: 620–629 Vargas et al IJROBP 2008; 70: pp. 744–751 University of Florida Dosimetry Data Show Protons Reduce Dose To The Rectum By 59% IJROBP 2008 Radiation dose to the rectum – proton therapy and IMRT1 Background on study Rectal Volume Receiving Radiation (%) 90% 80% IMRT 70% First prostate patients seen at University of Florida Proton Therapy Institute (“UFPTI”) Both proton and IMRT plans were planned prospectively for each patient The results 60% 50% Why this is important Dose to rectum is more than 2x with IMRT vs. protons at 32 Gy 40% 30% Dose to rectum is almost 2x with IMRT vs. protons at 70 Gy 20% Relative and absolute mean rectal dose savings of 59.2% and 20.1%, respectively, with proton therapy Proton Entire Dose Volume Histogram (“DVH”) does matter, not just high the dose region – Rectal wall volume irradiated at 32.4 Gy is biggest predictor of rectal toxicity2 Extremely high correlation between rectal volume irradiation to 70 Gy and 5-year toxicity rates3 10% 0% 0 (1) (2) (3) 10 20 30 40 50 60 70 Radiation Dose (CGE/Gy) 80 90 Carlos Vargas et al., “Dose-Volume Comparison of Proton Therapy and Intensity-Modulated Radiotherapy for Prostate Cancer,” International Journal of Radiation Oncology Biology Physics 70 No.3 (2008): 744-751. Susan Tucker, Lei Dong, Rex Cheung, et al., “Comparison of Rectal Dose-Wall Histogram Versus Dose-Volume Histogram for Modeling the Incidence of Late Rectal Bleeding After Radiotherapy,” International Journal of Radiation Oncology Biology Physics 60 (2004): 1589-1601. Mark Storey, Alan Pollack, Gunar Zagars et al., “Complications from Radiotherapy Dose Escalation in Prostate Cancer: Preliminary Results of a Randomized Trial,” International Journal of Radiation Oncology Biology Physics 48 (2000): 635-642. GI (Rectal) Side Effects and Complications The probability of damage to the GI tract is much higher with x-rays than protons Chronic Radiation Proctitis in the GI tract Inflammation caused by radiation 43 Necrosis and ulcer Dose Escalation Trials Support the Use of Protons for Prostate Cancer Protons offer better control and lower toxicity than X-Rays Randomized Boost Planning High 5-year Modality Technique dose arm control ≥G2 ≥G3 MD Anderson X-rays 2-D/3-D 78.0 Gy 78% 28% 10% CKVO96-10 X-rays 3-D 78.0 Gy 64% 32% 5% MRC RT01 X-rays 3-D 74.0 Gy 71% 33% 10% PROG 95-09 X-rays/Protons 3-D 79.2 Gy 92% 17% 1% trial1-4 GI toxicity The best outcome for control AND toxicity was achieved using protons (1) (2) (3) (4) (5) (6) DA Kuban, SL Tucker, L Dong et al., “Long-term results of the M.D. Anderson randomized dose-escalation trial for prostate cancer,” International Journal of Radiation Oncology Biology Physics 70 (2008): 67-74. (Note: toxicity updated from Viani et al, ref 6) ST Peters, WD Heemsbergen, PC Koper et al., “Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy,” 24 (2006): 1990-1196. DP Dearnaley, MR Sydes, JD Graham et al, “Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT101 randomized controlled trial,” Lancet Oncology 8 (2007): 475-487. Anthony L. Zietman, “Correction: Inaccurate analysis and results in a Study of Radiation Therapy in Adenocarcinoma of the Prostate,” JAMA 299 No. 8 (2008): 898-900. Anthony L. Zietman et al., “Comparison of Conventional-Dose vs. High-Dose Conformal Radiation Therapy in Clinically Localized Adenocarcinoma of the Prostate. A Randomized Controlled Trial,” JAMA 294 No. 10 (2005): 1233-1239. Beckendorf V, Guerif S, Le Prise E, et al. The GETUG 70 Gy vs. 80 Gy randomized trial for localized prostate cancer: Feasibility and acute toxicity. Int J Radiat Oncol Biol Phys 2004;60: 1056–1065. (Note: no 5-year control rates given) Viani GA et al. Higher-than-conventional radiation doses in localized prostate cancer treatment: a meta-analysis of randomized, controlled trials. Int J Radiat Oncol Biol Phys. 2009 Aug 1;74(5):1405-18. Reviewing the Data Parameter PROG 9509 MSK Collection Prospective Retrospective Institutions Multi-instituion Single-instituion Follow-up >10 year 8 years Photon RT 3D CRT IMRT Image Guidance? No Yes The Only Difference – Proton Boost i.e., this wasn’t even all protons – this was protons tacked onto what would be considered, by today’s standards, inferior radiation therapy Protons are Safer and More Effective A 2008 MGH study determined that protons decreases the risk of patients developing a secondary cancer by 50%(1) “According to the study, 6.4 percent of patients who underwent proton therapy developed a secondary cancer while 12.8 percent of patients who had photon treatment [x-rays] developed another type of cancer.” Protons significantly decrease the risk of secondary malignancies in prostate cancer treatment over 5 year period Modality Baseline risk2 4% Conventional3 10% IMRT4 Protons5 (1) (2) (3) (4) (5) Risk of Induced Tumor 11-15% 6% “Comparative Analysis of Second Malignancy Risk in Patients Treated with Proton Therapy versus Conventional Photon Therapy,” presented by Nancy Tarbell, M.D. at ASTRO 2008 (Chung et al. study) SEER data McGee et al., “Comparison of Second Cancer Risk in Prostate Cancer Patients Treated with Neutron/Photon Irradiation, Photon Irradiation, or Prostatectomy,” International Journal Radiation Oncology Biology Physics 66 (2006): S318-S319 Fontenot et al., “Risk of secondary malignant neoplasms from proton therapy and intensity-modulated x-ray therapy for early-stage prostate cancer,” International Journal Radiation Oncology Biology Physics 74 (2009): 616-622 Chung et al., “Comparative Analysis of Second Malignancy Risk in Patients Treated with Proton Therapy versus Conventional Photon Therapy,” International Journal Radiation Oncology Biology Physics 72 (2008) :S8 Prostate Cancer Summary Protons are AN option for prostate cancer treatment Protons are superior to IMRT Protons are different from surgery and brachytherapy Active surveillance is perfectly acceptable for many men with prostate cancer Discussions should be had with patients about ALL the options Parting Shots Take home points: All cancers should be approached in a multi-specialty or multi-disciplinary fashion Patient care should be performed in team approach: Concierge/Receptionists, Nurses, Therapists, Physicists/Dosimetrists, Physicians State of the Art Radiation Therapy @ CDH/Procure FULL Spectrum of Radiation Treatment options HDR Brachytherapy SBRT/SRS IMRT/3D CRT/IGRT Proton Beam Therapy Parting Shots Photons/Electrons will still be needed Brachytherapy will still be utilized Image guidance will remain critical for all modalities of radiation therapy Proton beam therapy can improve the side effects profile in many of the disease we currently treat with photon radiation. We are seeing just the tip of the iceberg Tumors we are and will be able to treat: Head / Neck • • Eye Sinus/nasal • Throat • Ear Pediatric • Brain • Spinal Cord • Bone Neurologic Other Solid Tumors • Brain • Breast Cancer (2011) • Spinal Cord • Lung Cancer (2011) • Colorectal Cancer • Prostate Questions