Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PowerPoint® Lecture Slides
prepared by
Betsy C. Brantley
Valencia College
CHAPTER
19
Development
and Inheritance
© 2013 Pearson Education, Inc.
Chapter 19 Learning Outcomes
• Section 1: An Overview of Development
• 19.1
• Discuss cleavage, blastocyst formation, and implantation of the
blastocyst in the uterine wall.
• 19.2
• Describe gastrulation and the formation and fate of the three
germ layers.
• 19.3
• Identify and describe the formation, location, and functions of
the extra-embryonic membranes.
• 19.4
• Discuss the importance of the placenta to the fetus during
prenatal development and as an endocrine organ.
© 2013 Pearson Education, Inc.
Chapter 19 Learning Outcomes
• 19.5
• Describe organogenesis and its role in the developing fetus.
• 19.6
• Describe the interplay between the maternal organ systems and
the developing fetus.
• 19.7
• List and discuss the events that occur during labor and delivery.
• 19.8
• Explain the milk let-down reflex and describe the five postnatal
life stages.
• 19.9
• Explain the role of hormones in males and females at puberty.
© 2013 Pearson Education, Inc.
Chapter 19 Learning Outcomes
• Section 2: Genetics and Inheritance
• 19.10
• Relate basic principles of genetics to the inheritance of human
traits.
• 19.11
• CLINICAL MODULE Identify several chromosomal disorders
and describe three tests performed during pregnancy used to
detect abnormal fetal development.
© 2013 Pearson Education, Inc.
Overview of Development (Section 1)
• Development
• Gradual modification of anatomical structures and physiological
characteristics from fertilization to maturity
• Divided into prenatal (before birth) and postnatal
• Prenatal development
• Embryological development
• Events occurring in first two months after fertilization
• Study of these events is embryology
• Fetal development
• Begins at start of ninth week and continues until birth
© 2013 Pearson Education, Inc.
Prenatal development
Prenatal Development
Embryological development
Fetal development
4 weeks
8 weeks
16 weeks
© 2013 Pearson Education, Inc.
Figure 19 Section 1 1 1
Gestation (Section 1)
•
Time spent in prenatal development
•
Usually divided into three trimesters (each three
months long)
1. First trimester
•
All major organ systems first appear
2. Second trimester
•
Development of all organ systems
3. Third trimester
•
© 2013 Pearson Education, Inc.
Most organ systems fully functional
Gestation or Prenatal Development (Section 1)
• Usually divided into three trimesters (each 3 months long)
1. First trimester
• All major organ systems first appear
2. Second trimester
• Development of all organ systems
• Body shape and proportions change
3. Third trimester
• Most organ systems fully functional
• Largest gain in fetal weight
© 2013 Pearson Education, Inc.
Postnatal Development (Section 1)
• Begins at birth and continues to maturity
• Maturity is state of full development and growth
• Basic understanding of prenatal and postnatal
development important
• Provides insights into anatomical structures
• Mechanisms of development and growth similar to
mechanisms for repair of injuries
© 2013 Pearson Education, Inc.
Day 0: Fertilization (19.1)
• Fertilization is fusion of two haploid gametes
• Enzymes released by multiple sperm create gap in follicular cells
and single sperm contacts oocyte membrane
• Sperm and egg nuclei (23 chromosomes each) fuse
• Produces zygote with 46 chromosomes
• Zygote then divides in process called cleavage
• Group of blastomeres created by cleavage called pre-embryo
• Cleavage lasts about seven days as pre-embryo travels down
uterine tube into uterus
© 2013 Pearson Education, Inc.
Development: Days 1–5 (19.1)
• First cleavage completed about 30 hours after fertilization
• Day 1: Two-cell stage
• Daughter cells (blastomeres) half size of zygote
• Day 2: Four-cell stage
• Two more daughter cells produced by second division
• Day 3: Early morula
• Pre-embryo now a solid ball of cells called morula
• Day 4: Advanced morula
• Morula reaches uterus by day 4
• Day 5
• Zona pellucida shed as morula enters uterus
© 2013 Pearson Education, Inc.
Cleavage and blastocyst formation
Day 3:
First Cleavage Day 1:
Day 2:
Two-Cell
Stage
Four-Cell Stage Early Morula
Division
Polar bodies
Blastomeres
Day 4:
Advanced Morula
Blastomeres
Day 5:
Loss of zona
pellucida and
transport to
uterus
Day 0: Fertilization
Start
Fertilization
Ovulation
© 2013 Pearson Education, Inc.
Figure 19.1
Development: Days 6–7 (19.1)
• Day 6: Blastocyst
• Blastomeres form a hollow ball (blastocyst) around an inner cavity
(blastocoele)
• Rate of growth increases and blastomeres no longer all identical in
size and shape
• Outer layer of cells (trophoblast) will provide nutrients to embryo
• Inner cell mass will form the embryo
• Day 7: Implantation
• Blastocyst attaches to endometrium, erodes endometrial lining, and
is enclosed within endometrium by day 10
© 2013 Pearson Education, Inc.
Development: Days 8–9 (19.1)
• Day 8: Trophoblast development
• Trophoblast cells divide rapidly
• Cells closest to blastocoele form cellular trophoblast
• Syncytial trophoblast
• Cells near endometrial wall lose plasma membranes, creating
layer of cytoplasm with multiple nuclei
• Day 9: Formation of amniotic cavity
• Fingerlike villi extend away from trophoblast into endometrium
creating channels called lacunae that fill with maternal blood
• Inner cell mass separates from trophoblast creating fluid-filled
chamber called amniotic cavity
© 2013 Pearson Education, Inc.
Implantation
Day 6: Blastocyst
FUNCTIONAL ZONE
OF ENDOMETRIUM
Uterine
glands
UTERINE
CAVITY
Blastocyst
Trophoblast
(outer layer
of cells)
Day 7: Implantation
Blastocoele
Inner
cell mass
Day 8: Trophoblast
Development
Syncytial
trophoblast
Day 9: Formation of
Amniotic Cavity
Cellular
trophoblast
Villi
Lacuna
Amniotic
cavity
Endometrial
capillary
© 2013 Pearson Education, Inc.
Figure 19.1
Module 19.1 Review
a. Define cleavage.
b. What developmental stage begins once the
zygote arrives in the uterine cavity?
c. Describe the blastocyst and its role in
implantation.
© 2013 Pearson Education, Inc.
Development: Days 9–10 (19.2)
• Day 9: Continued formation of amniotic cavity
• Inner cell mass organized into two layers, superficial and deep
• Cells from superficial layer migrate along walls of amniotic
cavity
• First step in formation of amnion, an extra-embryonic
membrane
• Day 10: Yolk sac formation
• Cells from deep layer of inner cell mass migrate around outer edge
of blastocoele
• First step in formation of yolk sac
• Yolk sac primary nutrient source for inner cell mass for next two
weeks
© 2013 Pearson Education, Inc.
Day 12: Gastrulation (19.2)
•
Some cells from superficial layer leave surface and move
between existing layers (superficial and deep)
•
Process called gastrulation
•
Creates three embryonic layers called germ layers
1. Ectoderm – superficial cells that didn't migrate
2. Endoderm – cells facing yolk sac
3. Mesoderm – migrating cells between endoderm and ectoderm
•
End result is oval, three-layered sheet called embryonic
disc
© 2013 Pearson Education, Inc.
Gastrulation
Day 9: Formation of Amniotic Cavity (continued)
ENDOMETRIUM
Inner cell mass
Superficial layer (blue)
Deep layer (orange)
Amniotic cavity
Blastocoele
Amnion
Cellular trophoblast
Day 10: Yolk Sac Formation
Syncytial trophoblast
Cellular trophoblast
Yolk sac
Lacuna
Day 12: Gastrulation
Yolk sac
Amnion
Ectoderm
Mesoderm
Primitive
streak
Blastodisc
Endoderm
Embryonic disc
© 2013 Pearson Education, Inc.
Figure 19.2
© 2013 Pearson Education, Inc.
Figure 19.2
Gestational Trophoblastic Neoplasia (19.2)
• Trophoblast divides rapidly and repeatedly and invades
tissue
• Also supposed to form extra-embryonic membranes
• In about 0.1 percent of pregnancies:
• Trophoblast behaves like a tumor
• Gestational trophoblastic neoplasia
• In 20 percent of cases, cells metastasize to other tissues and can
be fatal
• Treated with surgical removal of mass followed by chemotherapy
© 2013 Pearson Education, Inc.
Module 19.2 Review
a. Define gestational trophoblastic neoplasia.
b. Define gastrulation and describe its importance.
c. What germ layer gives rise to nearly all body
systems except the nervous and respiratory
systems?
© 2013 Pearson Education, Inc.
Four Extra-Embryonic Membranes (19.3)
•
Germ layers part of membrane formation
1. Yolk sac (endoderm and mesoderm)
2. Amnion (ectoderm and mesoderm)
3. Allantois (endoderm and mesoderm)
4. Chorion (mesoderm and trophoblast)
•
Membranes support embryological and fetal
development
© 2013 Pearson Education, Inc.
Yolk Sac (19.3)
• Begins as layer of cells around outer edges of
blastocoele
• Visible 10 days after fertilization
• Vascular network of yolk sac site of blood cell
formation
• Collects and distributes nutrients absorbed from
blastocoele
© 2013 Pearson Education, Inc.
Amnion (19.3)
• Begins as superficial cells migrate around amniotic
cavity
• Combination of mesodermal and ectodermal cells
• Amniotic fluid in amniotic cavity surrounds and
cushions developing embryo or fetus
© 2013 Pearson Education, Inc.
Formation of yolk sac and amnion
Formation of the
Yolk Sac
Endometrium
Formation of the
Amnion
Syncytial
trophoblast
Cellular
trophoblast
Layer of cells
that will become
yolk sac
Superficial cells
that will become
amnion
Blastocoele
Day 10
Syncytial
trophoblast
Cellular
trophoblast
Blastocoele
Completed
yolk sac
Amnion
(combination
of mesodermal
and ectodermal
cells)
Amniotic fluid
Day 14
© 2013 Pearson Education, Inc.
Figure 19.3
Allantois (19.3)
• Begins as outpocketing of endoderm near base of
yolk sac
• Free endodermal tip grows toward wall of
blastocyst, surrounded by mesodermal cells
• Extends partway into umbilical stalk
• Base of allantois will form urinary bladder
© 2013 Pearson Education, Inc.
Chorion and Placenta (19.3)
• Chorion
• Mesoderm associated with allantois spreads around
blastocyst, separating trophoblast from blastocoele
• Combination of mesoderm and trophoblast is chorion
• Beginning of the placenta
• Placenta
•
•
•
•
Forms from fetal and maternal cells
Villi of chorion invade endometrium
Primary support mechanism for developing embryo
Site of exchange (oxygen and nutrients for carbon
dioxide and wastes)
© 2013 Pearson Education, Inc.
Formation of allantois and chorion
Formation of the
Allantois
Formation of the
Chorion
Endometrium
Allantois
Chorion
Amniotic
cavity
Yolk
sac
Blastocoele
Embryo
Uterine lumen
Syncytial
trophoblast
Week 3
Umbilical
stalk
Allantois
Amniotic
cavity
Blastocoele
Embryo
Uterus
Uterine
lumen
Placenta
Yolk sac
Cervical
(mucous) plug
© 2013 Pearson Education, Inc.
Week 5
Figure 19.3
Module 19.3 Review
a. Name the four extra-embryonic membranes.
b. Which extra-embryonic membrane later gives
rise to the urinary bladder?
c. From which germ layers do the extra-embryonic
membranes form, and what are each
membrane's functions?
© 2013 Pearson Education, Inc.
Placenta Blood Supply (19.4)
• Umbilical arteries
• Carry blood from developing fetus to placenta
• Blood is deoxygenated and full of waste products
• Placenta
• Chorionic villi provide surface area for exchange of
gases, nutrients, and wastes
• Umbilical vein
• Carries blood from placenta back to fetus
© 2013 Pearson Education, Inc.
Placental structures with chorionic villus cross section
Area filled with
maternal blood
Trophoblast
Fetal blood
vessels
Umbilical
cord (cut)
Embryonic
connective
tissue
Yolk sac
Placenta
Chorionic villus,
cross section
LM x 280
Amnion
Chorion
Chorionic
villi
Endometrium
Myometrium
Area filled with
maternal blood
Uterine cavity
Cervical
(mucous) plug
in cervical
canal
External os
Cervix
Vagina
© 2013 Pearson Education, Inc.
Maternal
blood vessels
Umbilical Umbilical
vein
arteries
Amnion Trophoblast (cellular
and syncytial layers)
Figure 19.4 11
Placental structures with chorionic villus cross section
Umbilical
cord (cut) Yolk sac Placenta
Amnion
Chorion
Chorionic
villi
Endometrium
Myometrium
Uterine cavity
Cervical
(mucous) plug
in cervical
canal
External os
Cervix
Vagina
© 2013 Pearson Education, Inc.
Area filled with
maternal blood
Maternal
blood vessels
Umbilical Umbilical Amnion Trophoblast (cellular
and syncytial layers)
vein
arteries
Figure 19.4 11
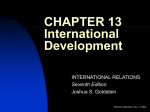
Placental Hormones (19.4)
• Human chorionic gonadotropin (hCG)
• Presence in blood or urine provides reliable indicator of
pregnancy
• Maintains corpus luteum and promotes continued
secretion of progesterone to maintain uterine lining
• Corpus luteum persists for three to four months before
declining in function
• Human placental lactogen (hPL)
• Helps prepare mammary glands for milk production
© 2013 Pearson Education, Inc.
Placental Hormones (19.4)
•
Relaxin
1. Increases flexibility of pubic symphysis allowing
expansion of pelvis during delivery
2. Causes dilation of cervix
3. Delays onset of labor contractions until late pregnancy
•
Progesterone and estrogen
•
After first trimester, progesterone from placenta
maintains endometrial lining
•
Estrogen production accelerates near end of third
trimester, playing role in stimulating labor and delivery
© 2013 Pearson Education, Inc.
Placental hormones
Placental Hormones
Human Chorionic Gonadotropin (hCG)
Human chorionic gonadotropin (hCG) appears in
maternal bloodstream soon after implantation and can
be tested for (in urine or blood) as an indicator of
pregnancy. hCG maintains the corpus leteum and
promotes continued secretion of progesterone.
Human Placental Lactogen (hPL)
Human placental lactogen (hPL) helps prepare the
mammary glands for milk production. At the mammary
glands, the conversion from inactive to active status
requires the presence of placental hormones (hPL,
estrogen, and progesterone) as well as several maternal
hormones (GH, prolactin, and thyroid hormones).
Relaxin
Relaxin is a peptide hormone that is secreted by the
placenta and the corpus luteum during pregnancy.
Relaxin (1) increases the flexibility of the pubic symphysis,
permitting the pelvis to expand during delivery; (2) causes
dilation of the cervix, making it easier for the fetus to enter
the vaginal canal; and (3) delays the onset of labor
contractions until late in the pregnancy.
Progesterone and Estrogen
After the first trimester, the placenta produces sufficient
amounts of progesterone to maintain the endometrial
lining and continue the pregnancy. As the end of the third
trimester approaches, estrogen production by the placenta
accelerates. As we will see in a later module, the rising
estrogen levels play a role in stimulating labor and delivery.
© 2013 Pearson Education, Inc.
Figure 19.4 22
Module 19.4 Review
a. Name the hormones synthesized by the syncytial
trophoblast.
b. The presence of which hormone in the urine
provides a reliable indicator of pregnancy in
home pregnancy tests?
c. When does the placenta become sufficiently
functional to continue the pregnancy?
© 2013 Pearson Education, Inc.
Organ System Formation (19.5)
• Process of organ formation is organogenesis
• Second week of development
• CNS forming
• Deep groove in ectodermal band along posterior midline
of embryo
• Fourth week of development
• Heart is beating
© 2013 Pearson Education, Inc.
Embryo in the second week of development
Future head of embryo
Thickened neural plate
(will form brain)
Central canal of future
spinal cord
Somites (mesodermal
blocks that will form
muscles and vertebrae)
Neural folds (fuse to
enclose brain ventricles
and central canal of
spinal cord)
Cut wall of
amnion
© 2013 Pearson Education, Inc.
Figure 19.5 11
Human development at four weeks
Medulla
oblongata
Ear
Forebrain
Eye
Heart
Body
stalk
Arm bud
Leg bud
Tail
© 2013 Pearson Education, Inc.
Figure 19.5 22
Organ System Formation (19.5)
• Sixth week of development
• Placenta has formed
• Embryo floating in amniotic cavity
• Limbs grow longer and skull bones form around brain
• End of first trimester
• Human features better defined
• Axial and appendicular muscles forming
• Fetal movements will begin soon
© 2013 Pearson Education, Inc.
Human development at six weeks
Chorionic villi
Amnion
Umbilical
cord
Placenta
© 2013 Pearson Education, Inc.
Figure 19.5 33
Human development at 12 weeks
Amnion
Umbilical
cord
© 2013 Pearson Education, Inc.
Figure 19.5 44
Fetal Development (19.5)
• After four months:
• Face and palate formed
• Cerebral hemispheres enlarging
• Hair follicles present and hair growing
• Peripheral nerves formed
• First eight weeks of fetal growth most rapid
• By end of second trimester, weighs about 0.64 kg
© 2013 Pearson Education, Inc.
Four month old fetus
© 2013 Pearson Education, Inc.
Figure 19.5 55
Fetal Development (19.5)
• Third trimester
• Organ systems become ready for normal function
• Rate of growth slows a little
• Largest weight gain in third trimester (about 2.6 kg) to
reach full-term weight of about 3.2 kg (7 lb)
© 2013 Pearson Education, Inc.
Ultrasound of six month old fetus
© 2013 Pearson Education, Inc.
Figure 19.5 66
Module 19.5 Review
a. Define organogenesis.
b. Identify the main event in fetal development
during the second trimester and third trimester.
c. During which trimester does the fetus undergo its
largest absolute weight gain?
© 2013 Pearson Education, Inc.
Maternal Changes with Pregnancy (19.6)
• Mother has to absorb enough oxygen, nutrients,
and vitamins for herself and fetus
• Must also eliminate all wastes generated
• Physical changes include:
• Weight gain of 6–7 kg
• Changes in balance since additional weight is not
evenly distributed
• Pushing maternal abdominal organs out of position
© 2013 Pearson Education, Inc.
Sectional view comparing organ positions in nonpregnant and pregnant women
Diaphragm
Liver
Stomach
Pancreas
Transverse
colon
Small intestine
Fundus of
uterus
Umbilical
cord
Placenta
Uterus
Urinary bladder
Pubic symphysis
Rectum
Urethra
Vagina
Nonpregnant female
© 2013 Pearson Education, Inc.
Cervical
(mucous)
plug in
cervical
canal
External
os
Pregnant female (full-term infant)
Figure 19.6 11
Maternal Physiological Adjustments (19.6)
• Increased respiratory rate and tidal volume
• To deliver extra oxygen and remove excess carbon
dioxide
• Almost 50 percent increase in maternal blood
volume
• To deliver blood to placenta and to compensate for
lowered oxygen levels in maternal blood
• Increased hunger sensations
• To meet increased requirements for nutrients, which can
be up to 30 percent above normal
© 2013 Pearson Education, Inc.
Maternal Physiological Adjustments (19.6)
• Increased maternal glomerular filtration rate (GFR) by 50
percent
• To eliminate additional wastes produced
• Increased frequency of urination
• In response to increased urine production and weight of uterus
pressing on urinary bladder
• Mammary gland development
• Fully developed and producing clear secretions by end of sixth
month
• Requires combination of hormones (hPL, prolactin, estrogen,
progesterone, GH, and thyroxine)
© 2013 Pearson Education, Inc.
Changes in the Uterus (19.6)
• Grows from 7.5 cm in length and 30–40 g in
weight to 30 cm in length and 1100 g in weight
• May contain up to 2 liters of fluid plus fetus and
placenta for total weight of 6–7 kg
• Number of uterine cells does not increase
• Expansion due to hypertrophy or enlargement of
existing cells, especially smooth muscle cells
© 2013 Pearson Education, Inc.
Physiological changes in maternal systems by end of third trimester
Maternal respiratory rate goes
up and tidal volume
increases.
Mammary glands are fully
developed by the end of the
sixth month of pregnancy.
Maternal glomerular filtration
rate increases by roughly 50
percent.
Maternal blood volume
increases by almost 50 percent
by the end of gestation.
Maternal requirements for
nutrients increases up to 30
percent above normal.
The uterus expands from 7.5
cm to 30 cm in length.
Because the volume of urine
produced increases and the
weight of the uterus presses
down on the urinary bladder,
pregnant women need to
urinate frequently.
© 2013 Pearson Education, Inc.
Figure 19.6 22
Pregnancy Risks (19.6)
• Pregnancy is a natural phenomenon yet not
without health risks
• Demands on maternal systems are possibly
dangerous
• Pregnant women over 35 are twice as likely to die
from pregnancy-related complications as from an
automobile accident
© 2013 Pearson Education, Inc.
Module 19.6 Review
a. List the major changes that occur in maternal
systems during pregnancy.
b. Why does a mother's blood volume increase
during pregnancy?
c. Based on the illustrations showing the locations
of the internal organs in nonpregnant and
pregnant women, explain why some women
experience difficulty breathing while pregnant.
© 2013 Pearson Education, Inc.
False and True Labor (19.7)
• Stretching of uterus causes gradual increase in
spontaneous smooth muscle contraction in myometrium
• Progesterone from placenta inhibits contractions in early
pregnancy
• False labor
• Spasms in uterine muscle that are not regular or persistent
• True labor
• Begins with series of events that are not reversible
© 2013 Pearson Education, Inc.
Position of fetus at onset of true labor
Placenta
Umbilical cord
Public
Vagina
symphysis
Cervical canal
© 2013 Pearson Education, Inc.
Cervix
Figure 19.7 11
Labor Initiation (19.7)
• Multiple factors responsible for beginning of true labor
• Placental factors include:
• Rising estrogen levels increasing muscle cells' sensitivity to
oxytocin
• Relaxin dilating cervix
• Release of maternal oxytocin stimulates smooth muscle contraction
• Contraction of myometrium distorts uterus, which stimulates more
oxytocin release
• Positive feedback continues until delivery is complete
© 2013 Pearson Education, Inc.
Factors involved in initiation of labor and delivery
Placental Factors
Placental estrogen increases the
sensitivity of the smooth muscle cells of
the myometrium and makes contractions
more likely. As delivery approaches, the
production of estrogen accelerates.
Estrogen also increases the sensitivity of
smooth muscle fibers to oxytocin.
Maternal Oxytocin Release
Maternal oxytocin release is
stimulated by high estrogen
levels. The smooth muscle in a
late-term uterus is 100 times
more sensitive to oxytocin than
the smooth muscle in a nonpregnant uterus.
Relaxin
produced by the
placenta relaxes
the pelvic
articulations and
dilates the ervix.
Distortion of Myometrium
Distortion of the myometrium
increases the sensitivity of
the smooth muscle layers,
promoting spontaneous
contractions that get
stronger and more frequent
as the pregnancy advances.
Labor contractions
move the fetus and
further distort the
myometrium. This
distortion stimulates
additional oxytocin
and prostaglandin
release. This positive
feedback continues
until delivery is
completed.
LABOR CONTRACTIONS OCCUR
© 2013 Pearson Education, Inc.
Figure 19.7 22
Stages of Labor (19.7)
•
Goal of labor is parturition: forcible expulsion of
fetus and placenta
•
Divided into three stages
1. Dilation stage
2. Expulsion stage
3. Placental stage
© 2013 Pearson Education, Inc.
Dilation Stage (19.7)
• Begins with onset of true labor
• Cervix dilates
• Fetus shifts toward cervical canal moved by
gravity and uterine contractions
• Lasts eight or more hours
• Contractions at the beginning last up to 30
seconds and occur once every 10–30 minutes
• Frequency and duration of contractions increase
• Amnion ruptures late in stage ("water breaks")
© 2013 Pearson Education, Inc.
Expulsion Stage (19.7)
• Begins as cervix completes dilation
• Contractions reach maximum intensity
• Can last up to full minute and occur two to three
minutes apart
• Stage continues until fetus has emerged from
vagina
• Usually lasts less than two hours
• Arrival of newborn outside mother's body is called
delivery
© 2013 Pearson Education, Inc.
Placental Stage (19.7)
• Uterine contractions continue
• Size of uterus decreases gradually
• Contractions tear connections between
endometrium and placenta
• Placenta or afterbirth is ejected
• Continued contractions after placenta ejected
compresses uterine blood vessels to restrict blood
loss
© 2013 Pearson Education, Inc.
Stages of labor
Dilation Stage
Expulsion Stage
Placental Stage
Uterus Ejection of the
placenta
© 2013 Pearson Education, Inc.
Figure 19.7 33
Premature Labor (19.7)
• When true labor begins before fetus has completed normal
development
• Chances of newborn surviving are directly related to body
weight at delivery
• Less than 400 g will not survive
• Respiratory, cardiovascular, urinary systems unable to support
life
• Less than 600 g (25–27 weeks) will not likely survive
• Premature delivery
• Birth at 28–36 weeks and weight over 1 kg
• With care, good chance of surviving and developing normally
© 2013 Pearson Education, Inc.
Module 19.7 Review
a. List and describe the factors involved in initiating
labor contractions.
b. What chemicals are primarily responsible for
initiating contractions of true labor?
c. Name the three stages of labor, and describe the
events that characterize each stage.
© 2013 Pearson Education, Inc.
Neonatal Period (19.8)
• Development continues after birth in the neonatal
period (first 28 days)
• Infancy is first year of life
• Dependent on mother for nourishment,
transportation, and protection
© 2013 Pearson Education, Inc.
Milk Production (19.8)
• By end of sixth month of pregnancy, mammary glands fully
developed and secreting colostrum
• Colostrum contains antibodies that help fight infection until
newborn's immune system develops
• Few days into nursing, mammary glands produce breast
milk
• Breast milk higher in fat content than colostrum
• Also contains antibodies and lysozyme (enzyme with antibiotic
properties)
• Breast milk provided to infants through milk let-down
reflex
© 2013 Pearson Education, Inc.
Milk Let-Down Reflex (19.8)
1. Stimulation by tactile receptors
•
Infant suckling
2. Neural impulse transmission to spinal cord and then to
brain
3. Stimulation of hypothalamic nuclei
•
Neurons in paraventricular nucleus
4. Oxytocin release at posterior lobe of pituitary gland
•
Hypothalamic neurons release oxytocin, which enters
bloodstream and circulates throughout body
5. Milk ejected
•
Oxytocin causes contraction of myoepithelial cells in walls
of lactiferous ducts and sinuses
© 2013 Pearson Education, Inc.
3
The milk let-down reflex
Stimulation of Hypothalamic
Nuclei
Posterior
lobe of the
pituitary
gland
4
5
Oxytocin Release
Milk Ejected
Start
© 2013 Pearson Education, Inc.
1
Stimulation of Tactile
Receptors
2
Neural Impulse
Transmission
Figure 19.8
1
Life Stages (19.8)
•
Five life stages in postnatal development
1. Neonatal period (first 28 days)
2. Infancy (first year)
•
Dependent on nutrition contained in milk
3. Childhood
•
Weaned from breast milk in early childhood
•
Body proportions gradually change
4. Adolescence
•
Begins at puberty, period of sexual maturation
•
Ends when growth is complete
5. Maturity
© 2013 Pearson Education, Inc.
Postnatal development
Postnatal Development
Neonatal Infancy
Childhood
Adolescence
Maturity
5 ft
4 ft
3 ft
2 ft
5
1 ft
0
1 month
© 2013 Pearson Education, Inc.
2 years
Puberty
(between)
9–14 years
18 years
Figure 19.8 22
Postnatal Hormonal Influences (19.8)
• Hormones affect tissues in specific ways
• Growth during infancy and childhood affected by:
• Growth hormone
• Adrenal steroids
• Thyroid hormones
• Adolescent growth and development
• Most affected by sex hormones
• Maturity
• Gradual changes associated with aging
© 2013 Pearson Education, Inc.
Module 19.8 Review
a. What hormone causes the milk let-down reflex?
b. Explain the difference between colostrum and
breast milk.
c. Name the stages of postnatal development, and
describe the time frame involved for each of the
stages.
© 2013 Pearson Education, Inc.
Hormonal Changes at Puberty (19.9)
•
Hypothalamus increases production of
gonadotropin-releasing hormone (GnRH)
•
Anterior pituitary gland responds by increasing FSH
and LH
•
In response, testicular or ovarian cells initiate:
1. Gamete production
2. Secretion of sex hormones, which stimulate
secondary sex characteristics and behaviors
3. Sudden acceleration in growth rate, ending with
closure of epiphyseal cartilages
© 2013 Pearson Education, Inc.
Responses to Testosterone in Males (19.9)
• Development of hairs on face and chest
• Terminal hair growth in axillae and genital area
• Accelerated bone deposition and skeletal growth
• Increased skeletal muscle growth and mass
• Activates central nervous system centers involved in
sexual drive and behavior
• Increased blood volume and hematocrit
• Thickening of larynx and lengthening vocal cords
• Functional development of accessory reproductive glands
and promotion of spermatogenesis
© 2013 Pearson Education, Inc.
Male responses to hormonal changes at puberty
Responses to Testosterone in Males
Integumentary System
Testosterone stimulates the development of hairs on the face and
chest, and stimulates terminal hair growth in the axillae and in the
genital area. Adipose tissues respond differently to testosterone
than to estrogen, and this difference produces the distinct
distributions of subcutaneous body fat in males versus females.
Skeletal System
Testosterone accelerates bone deposition and skeletal growth.
In the process, it promotes closure of the epiphyseal cartilages
and thus places a limit on growth in height.
Muscular System
Testosterone stimulates the growth of skeletal muscle fibers, and
the increased muscle mass accounts for significant sex differences in body mass, even for males and females of the same
height.
Nervous System
A surge in testosterone secretion at puberty activates the central
nervous system centers concerned with male sexual drive and
sexual behaviors.
Cardiovascular System
Testosterone stimulates erythropoiesis, thereby increasing
blood volume and the hematocrit.
Respiratory System
Testosterone stimulates disproportionate growth of the larynx and
a thickening and lengthening of the vocal cords. These changes
cause a gradual deepening of the voice in males.
Reproductive System
Testosterone stimulates the functional development of the
accessory reproductive glands, such as the prostate gland and
seminal glands, and helps promote spermatogenesis.
© 2013 Pearson Education, Inc.
Figure 19.9
Responses to Estrogen in Females (19.9)
• Continued development of fine vellus hairs
• Terminal hair growth in axillae and genital area
• Promotes initial development of mammary glands
• Causes more rapid epiphyseal closure
• Some stimulation of skeletal muscle fibers
• Activates central nervous system centers involved in sexual drive and
behavior
• Decreased plasma cholesterol levels
• Increased risk of iron-deficiency anemia due to iron loss with menses
• Thickening of myometrium and increased blood flow to endometrium
• Functional development of accessory reproductive structures
© 2013 Pearson Education, Inc.
Female responses to hormonal changes at puberty
Responses to Estrogen in Females
Integumentary System
Estrogen stimulates the hair follicles to continue to produce
fine vellus hairs and stimulate terminal hair growth in the
axillae and in the genital area. The combination of estrogen,
prolactin, growth hormone, and thyroid hormones promotes
the initial development of the mammary glands.
Skeletal System
Estrogen causes more rapid epiphyseal closure than does
testosterone. In addition, the period of skeletal growth is briefer
in females than in males, and so females generally do not grow
as tall as males.
Muscular System
Estrogen stimulates the growth of skeletal muscle fibers,
increasing strength and endurance, but not to the extent that
testosterone does in males.
Nervous System
A surge in estrogen secretion at puberty activates central
nervous system centers involved in female sexual drive and
sexual behaviors.
Cardiovascular System
The iron loss associated with menses increases the risk of
developing iron-deficiency anemia. Estrogen decreases plasma
cholesterol levels and slows the formation of plaque within
arteries. As a result, premenopausal women have a lower risk
of atherosclerosis than do adult men.
Reproductive System
Estrogen does not cause excessive growth of the larynx and
vocal cords, so females typically have higher-pitched voices
than males.
Reproductive System
Estrogen targets the uterus, promoting a thickening of the
myometrium and increasing blood flow to the endometrium.
Estrogen also promotes the functional development of
accessory reproductive structures in females.
© 2013 Pearson Education, Inc.
Figure 19.9
Module 19.9 Review
a. Name the three major interacting hormonal
events associated with the onset of puberty.
b. Why does a male generally have a deeper voice
and larger larynx than a female?
c. Why are premenopausal women at lesser risk of
atherosclerosis than men?
© 2013 Pearson Education, Inc.
Genetics (Section 2)
• Inheritance
• Transfer of genetically determined characteristics from
generation to generation
• Genetics
• Study of mechanisms responsible for inheritance
© 2013 Pearson Education, Inc.
Genotype and Phenotype (Section 2)
• Genotype
• Chromosomes and component genes
• Analogous to house architectural plan or blueprint
• Phenotype
• Anatomical and physiological characteristics displayed
by your pattern of genetic expression
• Analogous to physical appearance of a house
© 2013 Pearson Education, Inc.
Genotype versus phenotype
Genotype is like a set of
plans.
Phenotype is the detailed
structure.
© 2013 Pearson Education, Inc.
Figure 19 Section 2 1 1
Karyotype (Section 2)
• Entire set of chromosomes is a karyotype
• 23 pairs of chromosomes
• One member of pair came from spermatozoon
• Other member came from ovum
• Two together called homologous chromosomes
• 22 of the 23 pairs are autosomal chromosomes
• Genes affect somatic characteristics like eye color
• Last pair contains sex chromosomes
• Determines male (XY) or female (XX)
© 2013 Pearson Education, Inc.
Human karyotype
© 2013 Pearson Education, Inc.
Figure 19 Section 2 2 2
Homologous Pairs (19.10)
• Chromosomes in a homologous pair have same
structure and carry genes affecting same trait
• Genes found at same location or locus on each
chromosome
• Two chromosomes may carry same or different form
(allele) of gene
• If you have same allele, you are homozygous for trait
• If different alleles, you are heterozygous for trait
© 2013 Pearson Education, Inc.
Homologous autosomal pair of chromosomes
Homozygous (same
allele of a gene)
Heterozygous
(different alleles
for same gene)
© 2013 Pearson Education, Inc.
"Average"
autosomal pair
of chromosomes
contains about
1000 pairs of
alleles
Figure 19.10 11
Inheritance (19.10)
• Phenotype from a heterozygous genotype depends on how
corresponding alleles interact
• Most common form of interaction is simple inheritance
• Strict dominance
• Any dominant allele present is expressed in phenotype
• For example, even if you have only one allele for freckles, you
will show freckles
• "Freckle" allele dominant over "nonfreckle" allele
• Recessive allele only expressed if present on both
chromosomes of homologous pair
© 2013 Pearson Education, Inc.
Phenotype examples
© 2013 Pearson Education, Inc.
Figure 19.10 22
Punnett Squares (19.10)
• Dominant alleles indicated by capital letters
• Recessive alleles indicated by lowercase letters
• TT would be homozygous dominant
• Tt would be heterozygous
• tt would be homozygous recessive
• Punnett squares used to predict genetic probabilities
• In albinism example, if father homozygous (AA) for normal
pigmentation and mother homozygous (aa) for albinism, all children
will have genotype Aa and normal skin pigmentation
© 2013 Pearson Education, Inc.
Punnett squares
Maternal
a alleles a
A
Aa
Aa
A
Aa
Aa
Paternal alleles
(contributed
by sperm)
a
Aa
A
Paternal alleles
(contributed
by sperm)
a
© 2013 Pearson Education, Inc.
Maternal
alleles a
Aa
50% of the children are
heterozygous and have
normal pigmentation
aa
aa
50% of the children are
homozygous recessive
and have albinism
Figure 19.10 33
Polygenic Inheritance (19.10)
• Many phenotypic characteristics involve
interactions among several genes
• Polygenic inheritance
• Resulting phenotype depends on nature of alleles and
how those alleles interact with alleles from other genes
• For example, shading of brown or black hair color
© 2013 Pearson Education, Inc.
Example of polygenic inheritance
© 2013 Pearson Education, Inc.
Figure 19.10 44
Module 19.10 Review
a. Describe homozygous and heterozygous.
b. Differentiate between simple inheritance and
polygenic inheritance.
c. The trait "curly hair" operates through strict
dominance. What would be the phenotype of a
person who is heterozygous for this trait?
© 2013 Pearson Education, Inc.
Abnormal Chromosomes or Genes (19.11)
• Chromosomal abnormalities may involve
thousands of genes, so are usually lethal
• Variations in structure of individual genes are
relatively common
• More than 99 percent of human nucleotide bases
are the same in all people
• About 1.4 million single base differences or single
nucleotide polymorphisms (SNPs) exist
• Some associated with specific diseases
© 2013 Pearson Education, Inc.
Trisomy 21 (19.11)
• Down syndrome or trisomy 21 (three copies of
chromosome 21)
• Most common viable chromosome abnormality
• Causes mental retardation and physical malformations
• Degree of mental retardation ranges from moderate to severe
• Anatomical problems affecting cardiovascular system are often fatal
• In adulthood, many develop Alzheimer's disease before age 40
• Direct correlation between maternal age and risk of having child
with trisomy 21
• Risk increases from 1 in 2000 (before age 25) to 1 in 900 (ages
30–34) to 1 in 46 (ages 35–44)
© 2013 Pearson Education, Inc.
Trisomy 21
© 2013 Pearson Education, Inc.
Figure 19.11 11
Klinefelter Syndrome (19.11)
• Individual has sex chromosome pattern XXY
• Male phenotype but reduced androgen production
• Testes fail to mature (causing sterility)
• Breasts slightly enlarged
• Occurs in 1 in 750 male births
© 2013 Pearson Education, Inc.
Klinefelter syndrome
© 2013 Pearson Education, Inc.
Figure 19.11 22
Turner Syndrome (19.11)
• Individual has only single female sex chromosome (XO)
• Type of chromosomal deletion called monosomy
• Phenotype is normal female
• Estimated occurrence 1 in 2500 female births
• Maturation changes do not occur at puberty
• Ovaries nonfunctional with negligible estrogen production
• Physical abnormalities include short stature, low-set ears,
webbed neck
© 2013 Pearson Education, Inc.
Turner syndrome
© 2013 Pearson Education, Inc.
Figure 19.11 33
X-Linked Characteristics (19.11)
• X chromosome larger than Y chromosome
• Carries genes that affect somatic structures
• These genes called X-linked or sex linked
• No corresponding allele on Y chromosome
• Many associated with identifiable diseases or deficits
such as color blindness
© 2013 Pearson Education, Inc.
X-linked characteristics
X-linked allele
(allele not present
on Y chromosome)
Y
X
© 2013 Pearson Education, Inc.
Figure 19.11 44
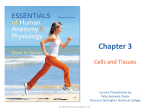
Color Blindness (19.11)
• Gene for distinguishing colors carried on X chromosome
• Males with dominant allele (XC) have normal color vision
• Males with recessive allele (Xc) have red–green color
blindness
• Females can have one dominant and one recessive allele
and still have normal color vision (XCXc)
• Females must have two recessive alleles to have red–
green color blindness (XcXc)
© 2013 Pearson Education, Inc.
Inheritance of an X-linked trait
A woman—who has two X chromosomes—
can be either homozygous dominant (XCXC)
or heterozygous (XCXc) and still have normal
color vision. She will be unable to distinguish reds from greens only if she carries
two recessive alleles, XcXc.
XC
A man has only one X
chromosome, so whichever
allele that chromosome carries
determines whether he has
normal color vision or is
red–green color blind.
Y
© 2013 Pearson Education, Inc.
XC
Xc
X C XC
XC Xc
Normal female Normal female
(carrier)
XC Y
Xc Y
Normal male
Color-blind
male
Figure 19.11 55
© 2013 Pearson Education, Inc.
Figure 19.11 66
Module 19.11 Review
a. Define single nucleotide polymorphism.
b. Name the disorder characterized by each of the
following chromosome patterns: (1) XO and (2)
XXY.
c. Why are X-linked traits expressed more
frequently in males than females?
© 2013 Pearson Education, Inc.