Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
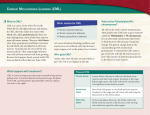
Anno accademico 2002-2003 Canale A: Prof. Malavasi Capitolo 10 La genetica del cancro Il cancro è una malattia genetica: 1) È il risultato di alterazioni nel DNA che alterano la regolazione del ciclo cellulare 2) Molte di queste alterazioni sono delle mutazioni 3) Le mutazioni possono essere causate da: - errori casuali nella replicazione - esposizione ai carcinogeni (per es. radiazioni o sostanze chimiche) - errori nel processo di riparazione del DNA Cancer is fundamentally genetic, in that it arises from mutations distorting the information contained in genes. At the same time, cancer is not genetic--the truly causative DNA damage is not inherited but acquired. D.W. Ross, Hospital Practice, 1999 Expanding the Basics 1) Cancer Arises from Damage to DNA. known causes of gene dysfunction include chemical or irradiational mutagenesis. Genomic flaws may also arise during DNA replication as errors that sometimes go undetected by intracellular repair mechanisms. In addition, certain viral infections are known to suppress gene function. 2) The Damage to DNA Is Acquired. Familial cases of cancer allow use of genetic mapping techniques to pinpoint cancer-related genes. 3) The Damage Typically Occurs in Multiple Steps. Epidemiologic data show that the incidence of cancer increases exponentially with age, but in a small proportion of cases, the damage happens to come fast, e.g. some leukemias The multi-hit hypothesis The Damage Affects Protooncogenes and Tumor Suppressor Genes. Our understanding of the molecular basis of cancer is built largely around evolving concepts of these two types of genes. So far, about 100 human protooncogenes have been discovered, and about 20 tumor suppressor genes. Both gene types specify proteins related to cell growth. A protooncogene product promotes such growth; a tumor suppressor gene product inhibits it. Oncogenes: -gain of function mutation: dominant -not heritable as a germline mutation Tumor suppressor genes: -loss of function mutation: recessive -heritable as germline mutation The example of follicular lymphoma Anno accademico 2002-2003 Canale A: Prof. Malavasi Capitolo 10 La genetica del cancro The example of chronic myeloid leukemia CML: clinical features 1) Clonal hematopoietic stem cell disorder 2) 20% of all leukemias (1 – 1,5 cases / 100,000) 3) Clinical course includes a chronic phase (4-5 yrs), an accelerated phase (6-18 mos) and a blast phase (3-6 mos) 4) Onset at >50 yrs CML: chronic phase 1) Characterized by mild hyperplasia with marked leukocytosis and immature cells of the granulocytic series 2) Lasts for approximately 4-6 yrs 3) Thrombocytosis and basophilia are common 4) Leukemic cells retain the capacity to differentiate normally 5) 50% of patients identified during routine blood tests 6) Main symptoms include fatigue, night sweats, abdominal discomfort due to splenomegaly CML: accelerated and blastic phases 1) Increasing myeloid immaturity; loss of the ability to differentiate normally 2) During the accelerated phase pts show a rising % of blasts (15-30%) and basophils (> 20%) in the PB and BM; 3) Blast phase can be either myeloid or lymphoid CML: molecular basis 1) 1960: Nowell and Hungerford described a consistent chromosomal abnormality in CML pts. 2) 1973: Rowley clarified that the shortened chr was the product of a reciprocal translocation 3) Majority of cases associated with (9; 22) (q34;q11) traslocation. It is a reciprocal translocation of the long arms of chromosome 9 and 22, resulting in a shortened chr 22 (the Philadelphia chr) 4) The molecular consequences is the fusion of the c-abl oncogene from chr 9 to sequences from chr 22, the breakpoint cluster region (bcr), giving rise to the bcr-abl gene. 5) The length of the fusion protein depends on the site of the breakpoint in bcr Why this chromosomal translocation? 1) Exposure to IR is a risk factor 2) Bcr and abl are in physical proximity in normal human cells 3) Bcr-abl transcripts are detectable at low frewuency in the blood of many healthy individuals 4) Why do some indivuals develop leukemia while others do not? - role of immune responses (HLA) - stage during which the translocation occurs CML: molecular features 1) The two most common fusion proteins are p185 and p210 2) p210 is seen in >95% of CML pts and 20% of ALL pts 3) p185 is seen in 10% of adult ALL pts and in the majority of pediatric Ph+ ALL pts 1) Ubiquitously expressed 145 kD protein, with 2 isoforms 2) Human homologue of the v-abl oncogene carried by the Ableson murine leukemia virus 3) Nonreceptor tyrosine kinase 4) Involved in regulation of cell cycle, in the cellular response to genotoxic stress, in the trasnmission of information concerning the environment through the integrin signaling pathway 1)160 kD protein, ubiquitously expressed 2) Serine threonine kinase activity in vitro (Bcr?) 3) Pleckstrin homology domain may activate nuclear factors 4) The true biological relevance remains to be determined The bcr-abl protein displays a deregulated tyrosine kinase activity Activation of mitogenic signaling The example of sqamous cell carcinoma of the cervix The retinoblastoma example The example of colon cancer 1) Second most common internal cancer 2) Accounts for 20% of cancer-related deaths in western countries 3) Incidence increases dramatically above age 50 4) Incidence approx equal in men and women 5) 5% is on a hereditary basis Hereditary colon cancer The example of breast cancer 1) 180,000 new cases each year in the US 2) 45,000 women die each year in the US because of breast cancer 3) 12% lifetime risk 4) 5-10% hereditary cases 5) Age and family history are the strongest risk factors Toward molecular cancer therapies 1. 2. 3. 4. Monoclonal antibodies: the example of anti-CD20 Antisense therapy Protein therapy Vaccines Antibody vs Tumor Signaling Apoptosis Cell cycle arrest Modulation Natural effectors Complement FcR bearing cells Induced anti-tumor response Antigen Exogenous effects R-active isotope toxins Potential resistance mechanisms to immunotherapy Lack or decreased expression of targeted antigen Expression of defensive antigens (CD46, CD55, CD59) Insufficient mAb delivery Delivery of apoptotic signals to effector cells Release of negative immunomodulators Antibody Specificity Target cell Type Edrecolomab (panorex®) Trastuzumab (Herceptin®) a-idiotype abs 17-1A colon/rectal cancer Murine IgG2a HER-2 breast cancer Humanized murine IgG1 individual B-cell tumor antigens CD52 CD20 B-cell lymphomas Customized human mAb CLL NHL Humanized IgG1 chimeric human/murine IgG1 B1 NHL Mouse HLA DR CD22 NHL NHL Murine IgG2a Murine IgG2a CD33 AML / CML humanized murine mAb CD20 NHL Chimeric human /murine IgG1 CAMPATH-1 Rituximab (Rituxan®) a-B1 (Tositumomab)* LYM-1* LL2 (Epratuzumab)*° a-CD33 (Hu-M195)* Ibritumomab * 131I-conjugated ° 90Y-conjugated Antisense therapy Gene therapy Towards molecular therapies


















































































![“Basic and translational oncology” [Selezionare la data] Italian](http://s1.studyres.com/store/data/003369983_1-0c2f97f3754c36ff0d6a75a322ab9225-150x150.png)








![Genistein [446-72-0] - Università degli Studi di Roma "Tor Vergata"](http://s1.studyres.com/store/data/001069358_1-826841ed5b5b39775155b3058987503a-150x150.png)