Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
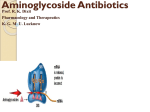
AMINOGLYCOSIDES The different members of this group share many properties in common. AMINOGLYCOSIDES Streptomycin Gentamicin Tobramycin Amikacin Netilmicin Kanamycin Neomycin AMINOGLYCOSIDES Amino sugars linked through glycosidic bonds. Polycations: This is in part responsible for many of their shared pharmacokinetic properties ANTIBACTERIAL ACTIVITY Primarily active against aerobic gram negative bacteria. Active against many staphylococci and certain Mycobacteria. Anaerobic bacteria are not susceptible. SENSITIVITY AND RESISTANCE AMINOGLYCOSIDE TRANSPORT Transport across the cell membrane is by active transport. Antimicrobial activity is reduced in an anaerobic environment and at low pH. RESISTANCE Cross-resistance occurs to varying degrees with the different aminoglycosides. Amikaciin ABSORPTION AND DISTRIBUTION Oral bioavailability is low. Once daily dosing (postantibiotic effect). Distribution into most body tissues including the CNS is low. EXCRETION Rapidly and almost entirely excreted by glomerular filtration (proportional to creatinine clearance). Accumulation occurs with impaired renal function. THERAPEUTIC USES Severe , complicated infections. Often combined with β-lactams. STREPTOMYCIN Bacterial endocarditis (combined with a penicillin or vancomycin). Tuberculosis. Gentamicin, Tobramycin, Netilmicin and Amikacin Similar in clinical indications and range of activity. Gentamicin is often preferred but resistance may limit its use. THERAPEUTIC USES Serious gram negative infections especially those due to Pseudomonas, Enterobacter, Klebsiella, Serratia etc. UTI’s, bacteremia, meningitis, infected burns, pneumonia, osteomyelitis, ear infections etc. THERAPEUTIC USES Severe Pseudomonas infections are best treated with one of these 4 AG’s plus an antipseudomonal penicillin or cephalosporin. Gentamicin combined with a penicillin is often used to treat bacterial endocarditis. THERAPEUTIC USES Tobramycin is often used in pseudomonal infections. Amikacin is used as the preferred agent in hospitals. Netilmicin- may be useful in resistant infections. DRUG INTERACTIONS Antipseudomonal penicillins inactivate aminoglycosides. Ethacrynic acid and other loop diuretics. Nephrotoxic agents. Neuromuscular blocking agents. SHARED PROPERTIES OF THE AMINOGLYCOSIDES Inhibit protein synthesis by binding to the 30S ribosomal subunit Pharmacokinetics-Poorly absorbed from the GI tract, Don’t get into the CNS very well, Rapidly excreted by kidney Toxicity-Ototoxicity, Nephrotoxicity, Neuromuscular blockade THERAPEUTIC USES OF THE AMINOGLYCOSIDES Streptomycin T.B., Endocarditis Gentamicin Endocarditis, gram negative infections, Pseudomonas Tobramycin Gram negative infections, Pseudomonas Amikacin Reserve drug for gram negativeinfections Nascent polypeptide chain 50S A Transferase site aa mRNA template P 30S Mechanism of action of Aminoglycosides AG’s Mature protein Blocks initiation Growing polypeptide 5’ 50S 3’ 30S AUG Wrong amino acid is incorporated 5’ mRNA translation 3’ Premature termination 5’ 5’ AUG 3’ X AUG + aminoglycoside Effects of Aminoglycosides 3’ Aminoglycosides on Protein Synthesis Mature Protein Growing Polypeptide 5’ AUG Blocks initiation 5’ 3’ Premature termination 3’ 50S 3’ 5’ X 30S + mRNA translation Amino Glycoside 5’ 3’ Incorporation of wrong amino acid MECHANISM OF ACTION Exact mechanism of cell death is unknown. Postantibiotic effect. RESISTANCE Alterations in ribosomal proteins. Decreased permeability to the antibiotic. TOXICITY Ototoxicity (Vestibular and Auditory). Nephrotoxicity. Neuromuscular Blockade. OTOTOXICITY The most serious toxic effect (uncommon, irreversible and cumulative). Caused by all the aminoglycosides OTOTOXICITY Several factors increase the risk. Careful monitoring is important. NEPHROTOXICITY Several factors may increase the risk. Reversible and usually mild. Reduced excretion can lead to ototoxicity. NEUROMUSCULAR BLOCKADE Rare but potentially serious. Occurs at high concentrations of aminoglycosides or in patients with an underlying risk factor. Acute neuromuscular blockade, respiratory paralysis and death can occur. TDH 7 /90 ves ci el cho lni e ace ty ltran s fe rase AC h AC h AC h A c e ty Cl oA + C h h gi h a ffni ity up take AC h AC h Amino Glycosides AC h AC h recep to r AC h A c +C h AC h es te ra se td h