Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
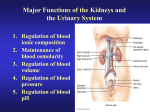
Anatomy of the Kidney, GFR and RBF Learning Objectives • Know the basic anatomy of the kidney and nephron. • Know how urine is transported to the bladder and the process of micturition. • Understand the relationship between filtration, reabsorption, secretion and excretion. • Understand the determinates of the glomerular filtration rate (GFR). • Know how afferent and efferent arteriolar resistances influence GFR and RBF. • Know how the juxtamedullary complex autoregulates GFR and RBF. Functions of the Kidneys • Excrete metabolic waste products, foreign chemicals, drugs and hormone metabolites. • Regulate H2O and electrolyte balances. • Regulate arterial pressure. • Regulate acid-base balance. • Release erythropoietin for erythrocyte production. • Produce vitamin D – important in Ca2+ regulation. • Regulate glucose synthesis. Gross Anatomy of the Kidney Renal Anatomy Nephron Anatomy Anatomy of the Urinary Bladder Transport of Urine from Kidney to Bladder •Stretching of the renal calyces induces peristaltic contractions that spread down the ureter and force urine into the bladder. •The ureter is constricted at the entrance to the bladder due to the basal tone of the detrusor muscle. The constriction prevents backflow of urine. •Peristaltic contractions in the ureter are enhanced by parasympathetic stimulation and inhibited by sympathetic stimulation. Micturition • Micturition is the process of emptying the urinary bladder. - As the bladder fills, stretch receptors initiate the micturition reflex. This causes contraction of the bladder, whose strength progressively increases. - Once the micturition reflex is stronger than the voluntary control of the external sphincter, urination occurs. Innervation and Anatomy of the Urinary Bladder Pelvic Nerves •Sensory nerves detect the degree of stretch in the bladder wall. •Parasympathetic motor nerves then cause contraction of the bladder. •Somatic nerves (pedendal) that control the voluntary skeletal muscle of the external sphincter. •Sympathetic nerves stimulate the bladder neck and external sphincter during filling (contraction). This is inhibited during micturition. Micturition Reflex •As pressure rises, stretch receptors begin to induce contractions via the parasympathetic nerves. •As the bladder fills, this reflex become more frequent and stronger. •When the bladder contains a lot of urine, a signal is also sent that inhibits the pedendal nerves. •If this last signal is more powerful than voluntary constriction of the external sphincter, urination occurs. Voluntary Urination • Contract abdominal muscles to increase pressure in bladder. • This excites the micturition reflex and inhibits the external sphincter. Factors of Urine Formation Renal Handling of Some Substances A. Waste products such as creatine. B. Many electrolytes. C. Nutritional substances, such as glucose and amino acids. D. Organic acids and bases, some foreign compounds and some drugs. Purpose of Reabsorption • Why filter, then reabsorb? - Control - High filtration rate makes it easy to remove waste products. - Reabsorption allows control of the body’s electrolyte balance. Volume of Filtered Plasma • ~20% of plasma flowing through a glomerular capillary is filtered. • In the average adult human, the glomerular filtration rate (GFR) for the kidney is 125 ml/min, or 180 L/day. • Entire plasma volume is ~3 L; so the entire plasma can be filtered ~60 times/day. Glomerular Capillary Membrane •Similar to fluid flow at other capillaries except, that the pores are larger. •Negative charge on the 3 layers of the capillary wall keep negatively charged albumin from being filtered. Determinants of GFR • As we discussed with other capillaries: - Glomerular hydrostatic pressure (PG). - Bowman’s capsule hydrostatic pressure (PB). - Glomerular colloid osmotic pressure (PGC). - Bowman’s capsule colloid osmotic pressure (PBC). • In addition, - Glomerular capillary filtration coefficient (Kf). - Kf is the product of the hydraulic conductivity and the surface area. • GFR – Kf(PG – PB – PGC + PBC) - PBC is normally considered to be 0. Net Filtration Pressure (excludes Kf) Capillary Filtration Coefficient • Kf is the product of the hydraulic conductivity and the surface area. - Hydraulic conductivity is the ease at which H2O flows through. • Kf is not measured directly, but calculated from Kf = GFR/Net filtration pressure • Kf does not normally change – IT’S A CONSTANT!! Bowman’s Capsule Hydrostatic Pressure • Increases would decrease GFR. • Normally not changed. • Obstructing urinary outflow can increase the hydrostatic pressure in Bowman’s capsule, as may occur with kidney stones. Glomerular Capillary Osmotic Pressure •PG changes during flow through glomerular capillary. •PG is increased by increasing filtration fraction and arterial osmotic pressure. •Filtration fraction is GFR/renal plasma flow. •Increased renal plasma flow decreases the filtration fraction. This causes a slower rise in the PG. •With a constant PG, an increase of BF into the glomerulus tends to increase GFR and viceversa. Glomerular Capillary Hydrostatic Pressure • Primary mechanism for physiological regulation of GFR, with increase in glomerular hydrostatic pressure, causing an increase in GFR. • 3 variables influencing glomerular hydrostatic pressure: 1. Arterial pressure; however, this is buffered by autoregulation (more later). 2. Afferent arteriolar resistance. 3. Efferent arteriolar resistance. Anatomy Reminder Changing Afferent and Efferent Arterioles Renal Blood Flow • RBF exceeds the kidney’s metabolic need, because of the need to filter the plasma. • RBF is determined with Ohm’s Law, which you already know. • Autoregulation keeps GFR and RBF, particularly GFR, fairly constant during changes in arterial pressure. Sympathetic and Humoral Control of GFR and RBF • Sympathetic nervous system constricts the vessels. Little influence at moderate stimulation. Important during severe stimulation, such as brain ischemia. • Norepinephrine and epinephrine – same as above. • NO provides a basal level of vasodilation. • Angiotensin II – constricts the efferent arteriole (more next lecture). Autoregulation of GFR and RBF What if GFR Increased with Arterial Pressure? GFR does not increase proportionally with arterial pressure (autoregulation) and reabsorption does increase with GFR. Autoregulation • There is a feedback mechanism that ensures a constant delivery of NaCl to the distal tubule. • This feedback mechanism, called tubuloglomerular feedback, is mediated by the macula densa in the juxtaglomerular complex. Juxtaglomerular Complex