Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
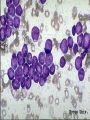
بنام خدا آنمی های شایع در کودکان DEFINITION OF ANEMIA : Anemia may be defined as a reduction in red blood cell mass or blood hemoglobin concentration. It is particularly important to use age and sex adjusted norms when evaluating a pediatric patient for anemia Normal limit of Hb in children: CLASSIFICATIONS OF ANEMIA : Physiologic classification Morphologic classification Mean corpuscular volume Blood loss (acute) Normal spleen, high retic count, normal bilirubin, normal urinalysis Hemolytic anemia Splenomegaly, Anemia Retic, bilirubin, spleen, U/A, increased reticulocyte count, high bilirubin (indirect), urobilinogen or hemoglobinuria Impaired red cell formation Normal spleen, low retic count, normal bilirubin, normal urinalysis Approch to anemia : blood loss(Acute): (Normal spleen, high retic count, normal bilirubin, normal urinalysis) Neonatal problem (fetofetal transfusion, fetomaternal transfusion,…) Hemorrhagic disease of newborn Meckel’s diverticulum, ….. Blood loss (acute) Anemia Hemolytic anemia Splenomegaly, increased reticulocyte count, high bilirubin (indirect), urobilinogen or hemoglobinuria Impaired red cell formation Approch to anemia: Hemolytic anemia (Splenomegaly, increased reticulocyte count, high bilirubin (indirect), urobilinogen or hemoglobinuria): 1) Corupuscular : Enzyme defect, Membrane defect, Hemoglobin disorder 2) Extra corpuscular immune, non immune Hemolytic anemia: Corpuscular 1) Enzyme defect: G6PD deficiency PK deficiency Glucose 6 phosphate dehydrogenase(G6PD) G6PD DEFICIENCY: X-linked disorder Affecting 200 to 400 million people Contains 515 amino acids Over 400 variant enzymes have been reported (90 according to specific mutations) Classification of G6PD variants: Class I variants: are rare, have severe enzyme deficiency (less than 10 percent of normal) and have chronic hemolytic anemia(44 variants) Class II variants : have severe enzyme deficiency, but there is usually only intermittent hemolysis (28 variants) Class III variants: have moderate enzyme deficiency (10 to 60 percent of normal) with intermittent hemolysis usually associated with infection or drugs (16 variants) Class IV variants: have no enzyme deficiency or hemolysis (2 variants) Class V variants: have increased enzyme activity PATHOPHYSIOLOGY OF G6PD DEFICIENCY: The in vivo half-life of enzyme: normal enzyme (G6PD B): 62 days, G6PD A- :13 days, G6PD Mediterranean: in hours G6PD A- : Patients usually have hemolysis that is mild and limited to older deficient erythrocytes (class III). G6PD B+(Mediterranean): red cells of all ages are grossly deficient (class II). DIAGNOSIS : Clinical presentation (should be considered in the differential diagnosis of any nonimmune hemolytic anemia) Laboratory findings: Hemolysis (Hb, Retic count, bilirubin, hemoglobinemia, hemoglobinuria), PBS (polychromatophlia,Heinz bodies, bite cells ),Rate of NADPH generation Hemolytic anemia: Corpuscular 1) Enzyme defect: G6PD deficiency PK deficiency Pyruvate kinase deficiency : Clinical presentation : a broad spectrum of clinical and hematologic findings occurs, ranging from a mild, completely compensated hemolytic state to severe anemia. Anemia and hyperbilirubinemia may occur in the neonatal period. In the older patient, pallor, scleral icterus, and splenomegaly are usual findings. Pyruvate kinase deficiency : Laboratory findings : Elevated reticulocyte count. A few small spiculated erythrocytes No increased number of spherocytes Osmotic fragility is normal. Hemolytic anemia: Corpuscular 1) Enzyme defect 2) Membrane defect: Spherocytosis, Elliptocytosis Membrane defect :Spherocytosis Pathophysiology : A deficiency or abnormality of the erythrocyte membrane structural protein: spectrin , ankyrin, band 3, and protein 4.2. The spherocyte is relatively rigid and nondeformable Membrane defect :Spherocytosis Clinical presentation: anemia, hyperbilirubinemia, splenomegaly Expansion of the marrow cavities . Laboratory findings reticulocytosis, anemia, hyperbilirubinemia, spherocyte in PBS, Erythroid hyperplasiain BMA, osmotic fragility test, Autohemolysis, Hemolytic anemia: Corpuscular 1)Enzyme defect 2) Membrane defect 3) Hemoglobin disorder Normal variant, Functional disorder, Structural problem, Thalassemia Hemolytic anemia: Hemoglobin disorder: Normal variant, Functional disorder, Structural problem, Thalassemia عوارض کم خونی تغییرات استخوانی بزرگی طحال خون سازی خارج مغز استخوان شکستگی پاتولوژ یک افت سطح هوشی زخم اندام تحتانی توقف رشد عوارض سیستم انعقادی Hemolytic anemia: Extracorpuscular Immune: Nonimmune: Alloimmune, isoimmune, Autoimmune HUS syndrome, TTP, DIC, Infection, Burn, Hypersplenism, …….. Typical Hemolytic Uremic Syndrome: In the majority of cases, Stx HUS is associated with strains of Escherichia coli that produce a Shiga toxin D+ HUS associated with Shigella dysenteriae serotype 1 will be included in the discussion of Stx HUS Cases of HUS in children due to Shiga toxinproducing E. coli infections other than colitis (e.g. UTI) can occur . Blood loss (acute) Anemia Hemolytic anemia Impaired red cell formation Normal spleen, low retic count, normal bilirubin, normal urinalysis Approch to anemia : Impaired red cell formation (Normal spleen, low retic count, normal bilirubin, normal urinalysis) 1)Deficiency Iron deficiency Megaloblastic anemia vitamins, Thyroxine deficiency 2)Bone marrow failure Failure of a single cell line Failure of all cell line: 3)Bone marrow infiltration Malignant: Non malignant: Approch to anemia : Impaired red cell formation (Normal spleen, low retic count, normal bilirubin, normal urinalysis) 1)Deficiency Iron deficiency Megaloblastic anemia vitamins Thyroxine deficiency 2)Bone marrow failure 3)Bone marrow infiltration Clinical manifestation of IDA; Hematological symptoms The most common presentation of IDA is an otherwise asymptomatic, well nourished infant or child who has a mild to moderate microcytic, hypochromic anemia Clinical manifestation of IDA; Non hematological symptoms Neurodevelopmental and Cognitive function Immunity Exercise capacity Pica and pagophagia Thrombosis Epithelial change: dysphagia, esophageal web, atrophic glossitis, spoon nails, blue sclerae Approch to anemia : Impaired red cell formation (Normal spleen, low retic count, normal bilirubin, normal urinalysis) 1)Deficiency 2)Bone marrow failure Failure of a single cell line : CPRA, TEC, A.crisis Failure of all cell line: Aplastic anemia 3)Bone marrow infiltration Fanconi Anemia: Clinical features Incidence is 3/1,000,000 – Heterozygote frequency ~1/300 in U.S. and Europe Median age at diagnosis is 5-7 Median survival is 20-30 yrs. Phenotypic variability occurs even within families Frequency of abnormalities in FA Abnormality Frequency (%) Skeletal (radial ray, hip, vertebral scoliosis, rib) 71 Skin pigmentation (café au lait, hyper- and hypopigmentation) 64 Short stature (median height 5th %ile) 63 Eyes (microphthalmia) 38 Renal and urinary tract 34 Male genitalia 20 Mental retardation 16 Gastrointestinal (eg, anorectal, duodenal atresia) 14 Cardiac abnormalities 13 Hearing 11 Central nervous system (eg, hydrocephalus, septum pellucidum) 8 No abnormalities 30 Approch to anemia : Impaired red cell formation (Normal spleen, low retic count, normal bilirubin, normal urinalysis) 1)Deficiency 2)Bone marrow failure 3)Bone marrow infiltration Malignant: Leukemia… Non malignant: Metabolic disease Osteopetrosis Fast Cases A 15 yo girl with a history of systemic lupus erythematosus comes to the clinic for evaluation of fatigue and pallor. Hgb is 7.2, MCV 85, Retic 10%, WBC 3.5 (50% polys, 40% lymphs, 10% atypicals), and plts of 125. The smear shows microspherocytes and rouleaux formation. She does not have a history of blood loss. What does she have? Autoimmune hemolytic anemia 17 mounts age infant with an unexplained persistent anemia History of neonatal jaundice Requirement of pRBC transfusion * 2 early infancy Hb stable 7-9 gr/dl from age 3-17 months spleen 5 cm below costal margin Retic 20%, with indirect hyperbilirubinemia What does she have? Pyruvate kinase deficiency A 3 yo girl has had diarrhea, sometimes bloody, for several days. Now, she has fever, edema, petechiae & hypertension. The CBC shows: Hgb 7.5, MCV 79, Retic 15%, Plts 35, and WBC 13.5 with a normal differential. The smear shows several helmet cells and polychromasia and confirms the thrombocytopenia What does she have? Hemolytic uremic syndrome A 3 month old boy is brought to the ED lethargic and with a fever of 40° C. While attending to the airway, correcting hypotension and initiating antibiotics, the nurse informs you of the CBC results: Hgb 5.8, MCV 81, Retic 16%, WBC 23.5 (56% polys, 24% bands, 10% lymphs, & 10% atypical lymphs) and plts of 350. He has blood on dipstick analysis of his urine with no RBC’s on microscopic analysis. The blood shows polychromasia, and several bite cells. What does he have? G6PD deficiency A 9 month old boy comes the Dr.’s office for evaluation of a cold. Further hx reveals introduction of whole cow’s milk at 5 months and no well baby visits. He appears quite pale and has the following findings: Hgb 5.3, MCV 48, plts 780, WBC 12.5 and retic 1.7% What does he have? Iron Deficiency anemia An 18 month old girl was in good health until she developed a cold 10 days ago. Now she is pale but without visible jaundice. The CBC shows a Hgb of 6.8, MCV of 78 and retic of 0.1%, WBC & Plts are normal as is the peripheral blood smear. What does she have? Transient Erythroblastopenia Childhood of The CBC of an 8 yo girl reveals the following: Hgb 10, MCV 102, Retic 0.4%, WBC normal, Plts 125. She is slightly short, has several large café-au-lait spots, is performing below average in school and has short thumbs. What does she have? Fanconi’s Anemia You are asked to assist in the care of political refugees from Afghan. On the screening entrance exam you note that one of them, a 2 yo girl, is very pale and lethargic. Her spleen is down to the level of the umbilicus. The labs reveal: Hgb 6.3, Retic 6%, MCV 55, with normal WBC & plts. The smear shows many target cells, polychromasia, basophilic stippling, red cell fragment, anisocytosis and hypochromia. What does she have? thalassemia major People may doubt what you say but they will believe what you