Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
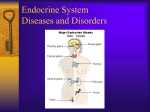
Evaluating Outcomes for Clients with Thyroid and Parathyroid Problems Hyperthyroidism Thyrotoxicosis Graves’ disease, the most frequent causes: goiter, exophthalmos, pretibial myxedema Laboratory assessment Thyroid scan Ultrasonography Electrocardiography Drug Therapy Radioactive iodine therapy; not used in pregnant women – Additional drug therapy may be needed. – Implement radiation precautions. – Monitor regularly for changes in thyroid function. Surgical Management Surgery possible in absence of good response to drug therapy. Postoperative care for: – Hemorrhage – Respiratory distress – Hypocalcemia and tetany – Laryngeal nerve damage – Thyroid storm or thyroid crisis Infiltrative Opthalmopathy Provide symptomatic treatment. Treatment of hyperthyroidism does not correct eye and vision problems of Graves’ disease. Elevate the head of bed at night. Instill artificial tears. Treat photophobia with dark glasses. (Continued) Infiltrative Opthalmopathy (Continued) Give steroid therapy. Provide diuretics. Hypothyroidism Decreased metabolism from low levels of thyroid hormones Myxedema coma a rare, serious complication Mostly a result of thyroid surgery and radioactive iodine treatment of hyperthyroidism Clinical manifestations Decreased Cardiac Output Interventions: – Monitor circulatory status. – Monitor for signs of inadequate tissue oxygenation. – Monitor for changes in mental status. – Monitor fluid status and heart rate. – Administer oxygen or mechanical ventilation, as appropriate. Ineffective Breathing Pattern Interventions: – Observe and record rate and depth of respirations. – Auscultate the lungs. – Assess for respiratory distress. – Assess the client receiving sedation for respiratory adequacy. Disturbed Thought Processes Interventions: – Assess lethargy, drowsiness, memory deficit, poor attention span, and difficulty communicating. – These problems should decrease with thyroid hormone treatment. – Provide a safe environment. – Provide family teaching. Myxedema Coma Coma, respiratory failure, hypotension, hyponatremia, hypothermia, hypoglycemia Emergency care Thyroiditis Inflammation of the thyroid gland Three types of thyroiditis: acute, subacute (granulomatous), and chronic (Hashimoto’s disease)—the most common type Dysphagia and painless enlargement of the gland Nonsurgical management, drug therapy Surgical management Thyroid Cancer Papillary, follicular, medullary, and anaplastic Collaborative management Surgery treatment of choice: thyroidectomy Suppressive doses of thyroid hormone for 3 months after surgery Study performed after drugs are withdrawn Hyperparathyroidism Parathyroid glands: calcium and phosphate balance Hypercalcemia and hypophosphatemia Nonsurgical management: – Diuretic and fluid therapy – Drug therapy: phosphates, calcitonin, calcium chelators Surgical Management Parathyroidectomy care: preoperative – Client stabilized; calcium levels normalized – Studies: bleeding and clotting times, CBC – Teaching: coughing, deep-breathing exercises, neck support Operative procedures (Continued) Surgical Management (Continued) Postoperative care includes: – Observe for respiratory distress. – Keep emergency equipment at bedside. – Hypocalcemic crisis can occur. – Recurrent laryngeal nerve damage can occur. Hypoparathyroidism Decreased function of the parathyroid gland Iatrogenic hypoparathyroidism Idiopathic hypoparathyroidism Hypomagnesemia Interventions: correcting hypocalcemia, vitamin D deficiency, and hypomagnesemia If a manifestation is caused by hyperthyroidism, indicate “HYPER”. If a manifestation is caused by hypothyroidism, indicate “HYPO.” Tremors Heat intolerance Weight gain Tachycardia Insomnia Dry, coarse, brittle hair Decreased activity tolerance Decreased body temperature Palpitations Apathy Diaphoresis Thinning of scalp hair Thick, brittle nails Constipation HYPO = Hypothyroidism HYPER = Hyperthyroidism Tremors: HYPER Heat intolerance: HYPER Weight gain: HYPO Tachycardia: HYPER Insomnia: HYPER Dry, coarse, brittle hair: HYPO Decreased activity tolerance: HYPO Decreased body temperature: HYPO Palpitations: HYPER Apathy: HYPO Diaphoresis: HYPER Thinning of scalp hair: HYPER Thick, brittle nails: HYPO Constipation: HYPO Myxedema During hypothyroidism, cellular energy production is decreased and metabolites build up. The metabolites are compounds of proteins and sugars called glycosaminoglycans. These compounds build up inside cells, which increases mucous and water, forms cellular edema, and changes organ texture. The edema is mucinous edema (called myxedema) rather than edema caused by water alone. Myxedema Coma A rare, serious complication of untreated or inadequately treated hypothyroidism. Decreased metabolism leads to a flabby heart increased chamber size Cardiac output decreases Perfusion to the brain and other organs decreases Decreased perfusion makes slowed cellular metabolism worse. Tissue and organ failure occurs. Causes of hyperparathyroidism include the BOLD items: Congenital dysgenesis Parathyroid carcinoma Vitamin D deficiency Hypomagnesemia Chronic renal failure with hypocalcemia. Neck trauma Other causes are parathyroid adenoma, congenital hyperplasia, neck radiation, parathyroid hormone-secreting carcinomas of lung, kidney , or GI tract.