Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
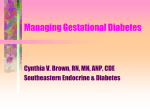
Pramlintide Therapy Part 2 of 2 Pharmacodynamic Review Type 1 Diabetes Efficacy Safety Severe Hypoglycemia Annual Event Rate by Dose Type 1 Diabetes Weeks 0-4 5 4 Mean (SE) 3 Event Rate Per Subject 2 Year 1 0 Placebo + Ins Pram 30 QID + Ins Pram 60 TID + Ins Pram 60 QID + Ins Pram 90 BID + Ins Pram 90 TID + Ins Risk for Severe Hypoglycemia Decreases over Time Type 1 Diabetes, All Patients 0.06 Placebo + Insulin Pramlintide + Insulin 0.05 Risk 0.04 0.03 0.02 0.01 0.00 2 4 6 8 10 12 14 16 RT O’Neill Drug Information Journal; 21: 9-20, 1987. 18 20 22 24 26 28 30 Weeks 32 34 36 38 40 42 44 46 48 50 52 Pramlintide Benefits are Seen in Patients with Type 1 Diabetes Targeting Optimal Glycemic Control 8 Mean HbA1C (%) 7.8 7.6 7.4 7.2 4 6 8 Time (Weeks) 4.5 Weight Insulin Use 6 4 2 0 10 12 14 16 18 20 22 24 26 1 0 -1 -2 -3 Event Rate Per Subject Year 2 Change in Weight (lb) Change in Insulin Use (%) 0 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 Pramlintide (n=243) Placebo (n=173) Severe Hypoglycemia Weeks 0-4 Weeks 4-26 Other Safety Observations Type 1 Diabetes No evidence of: – Serious events that are unusual in the absence of drug therapy – Cardiac toxicity – Hepatic toxicity – Renal toxicity No increase in frequency of clinically significant: – Lipid abnormalities – ECG changes – Changes in vital signs Systolic blood pressure Diastolic blood pressure – Laboratory abnormalities Pramlintide is Efficacious and Safe in Type 1 Diabetes Improves glycemic control Weight loss Increased insulin-induced hypoglycemia only during initiation of therapy – No increase in insulin-induced hypoglycemia after initiation of therapy No other safety issues Dosage recommendation: – Initiate at 30 µg 3-4 times/day before meals – Maintenance 30 or 60 µg 3-4 times/day before meals Guidelines for Initiation of Therapy Initial Dose – Type 2: 120 µg – Type 1: 30 µg or lower Dose Frequency – Determined by meal pattern – Administered within 15 minutes before a meal Insulin Reduction – 10%-20% of preprandial, short-acting insulin dose For use with meal time insulin Pramlintide Approved for those using insulin and not at goal Used only with insulin to lower BG after meals Only given at mealtimes Increases risk for Hypoglycemia Patient must check before/after meals and bedtime Rapid insulin dose reduced 50% Will help lose weight Most common side effect is Nausea-dose related Cannot mix with insulin Must be titrated to lessen nausea Starting dose 15micrograms increasing gradually to a max of 120ug Must not use if eating less then 250 calories or 30gm carbs No driving until regulated Reduces caloric intake, delays food adsorbtion lowering PPBG and reduces Glucagon secretion.