Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Orphan drug wikipedia , lookup
Compounding wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Psychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Plateau principle wikipedia , lookup
Prescription costs wikipedia , lookup
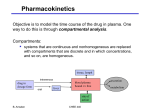
Part 2 Pharmacokinetics 药物代谢动力学 Kinetics Models Parameters 2. Transport of Drug in the Body A. aqueous B. lipid cell channels in the membranes intercellular junctions C. carriers (transporters) (into or out of cells) D. endocytosis exocytosis Mechanisms of drug permeation across cell membrane 2.1 Transmembrane Transport of Drugs (1) Non-carrier Transport Simple diffusion(简单扩散/单纯扩散) Filtration(滤过) (2) Carrier-mediated Transport a. Active transport Characteristics of active transport Involving specific carrier (transporter) Energy-dependent Saturability Competition at same carrier Moving against concentration gradient (up-hill) b. Facilitated diffusion(易化扩散) (transporter-mediated diffusion) Involving specific carriers (transporter) Energy-independent Saturability Competition with other drugs Concentration gradient (down-hill) (3) Endocytosis/exocytosis(入胞/出胞) Another classification Passive transport Simple diffusion(简单扩散/单纯扩散) Filtration(滤过) Facilitated diffusion(易化扩散) Active transport Active transport (主动转运) Pinocytosis/exocytosis(入胞/出胞) A. Simple diffusion Most drugs are weak acids or bases. Their diffusion passing through cell membrane depends the lipid-soluble state (un-ionized form) Determinants of simple diffusion For most drugs of small molecules (usually are weak acids or weak bases): Lipid-soluble or un-ionized forms pKa of the drug and pH of the body fluid The pKa is the pH at which the concentrations of the ionized and un-ionized forms are equal. Henderson-Hasselbalch equation Weak acid drugs: pH - pKa = log ( [A-] / [HA] ) pKa - pH = log ( [HA] / [A-] ) Weak base drugs: pKa - pH = log ( [BH+] / [B] ) pH - pKa = log ( [B] / [BH+] ) pH pKa Weak acids And / or Weak bases And / or And / or And / or un-ionized form lipidsoluble Simple diffusion B. Carrier (transporter)-mediated transport Three types of functional membrane proteins. Models of transmembrane transport across the lipid bilayer 2.2 Free and Bound Forms Plasma protein binding Tissue / organ affinity 3. Fate of the drug in the body Absorption Distribution Metabolism (Biotransformation) Excretion - ADME ADME 3.1 Absorption Absorption is the transfer of a drug from its site of administration to the blood stream. Gastrointestinal tract Parenteral injection - i.m., s.c. Inhalation Transdermal (1) Gastrointestinal tract Route: Oral Sublingual Rectal Absorption sites: Oral Gastric Intestinal Rectal Factors influencing absorption: blood flow to the absorption site total surface area available for absorption contact time at the absorption surface physic-chemical properties of the drug first-pass elimination (2) Parenteral injection intramuscular injection ( i.m. ) subcutaneous injection ( s.c. ) Determinants Local blood flow; Solubility of the drug (3) Others Inhalation; Intranasal; Transdermal; Topical 3.2 Distribution Drug distribution is the process by which a drug reversibly leaves the blood stream and enters the interstitium (extracellular fluid) and / or the cells of the tissues. Blood flow-dependent phase of distribution Selective distribution Tissue-plasma balance: importance of measuring plasma concentration (1) Binding of drug to plasma proteins Bound drug: can not distribute / inactive temporally reversible (storage form) / percentage of binding plasma protein capacity competitive displacement (2) Physic-chemical properties of the drug (3) Blood flow and re-distribution (4) Affinity to organs or tissues (5) Barriers Blood-brain barrier (BBB) Placental barrier Blood-eye barrier Blood-brain barrier (BBB) Able to pass through Unable to pass through Small molecules Large molecules Lipid-soluble Water-soluble Transporter-mediation Amount of drug passing through BBB Increases when inflammation or larger doses used Placental barrier: More permeable Drugs for pregnant women: A, B – relatively safe C - caution D, X - toxic 3.3 Metabolism (biotransformation) Drug metabolism is the process transforming lipophilic drug into more hydrophilic metabolites, which is essential for the elimination of these compounds from the body and termination of their biological activity. (1) Metabolism sites Liver: for most of the drugs Other organs/tissues: intestine, kidney, lung, plasma, etc. (2) Phases of metabolism Phase I: Oxidation, reduction, hydrolysis most drugs are inactivated few (prodrugs) is activated Phase II: Conjugation inactivated Metabolites: more water-soluble easier to excrete (3) Enzymes in drug metabolism Enzymes in Phase I: cytochrome-P450, such as CYP2A6, CYP3A4 many other enzymes Enzymes in Phase II: acetylase glucuronosyltransferase etc. Induction of hepatic enzymes by drugs example: phenytoin-steroids, nifedipine Inhibition of hepatic enzymes by drugs example: verapamil-diazepam 3.4 Excretion Removal of a drug from the body via a number of routes. Elimination of drugs from the body Action on excretory organs 3.4 Excretion (1) Excretion routes Kidney -renal excretion Bile (hepato-enteral circulation) Lung GI tract Milk Secretion glands 3.5 Elimination and Accumulation Elimination(消除) Metabolism Excretion Distribution (stored in fat, hair, etc) Accumulation(蓄积) Dosing rate > elimination rate Kinetic Processes Kinetics Models Parameters 1. 2. 3. 4. Drug concentration-time curve (C-T curve) Kinetic rate processes Pharmacokinetic models Pharmacokinetic parameters and their implications Kinetic Processes 1. Drug concentration-time curve (C-T curve) Maximal (peak) concentration: Cmax or Cp Time to maximal concentration (Peak time ) : Tmax or Tp Area under the curve: AUC Multiple dosing (steady state): Css max, Css min, Css C ← i.v. i.m. ← Cmax ← Cp s.c. Oral ↑ ↑ ↑ Tmax, Tp ← t C ←Cmax AUC ↑ Tmax t Tmax, Cmax and AUC C-T curve after multiple dosing (same dose and interval) 在临床治疗中多数药物通过重复给药以期达到有效治疗血药浓度,并维持 在一定水平,此时给药速率与消除速率达到平衡,其血药浓度称为稳态浓 度,用Css表示 2. Kinetic rate processes dC / dt = -KCn 2.1 Zero order kinetics n=0 dC / dt = -K Ct = C0-K t C0-Ct = K t when Ct=1/2 C0, t = t1/2 then, 0.5 C0 =K t1/2 t1/2=0.5 C0 / K Zero order kinetics A. same amounts of drug are eliminated per unit time B. t1/2 is not a constant C. C-T curve is linear D. no Css theoretically Kinetic properties of C-T curves after single bolus injection of drug 2.2 First order kinetics n=1 dC / dt = -KC Ct = C0e-Kt lnCt = lnC0-Kt Kt=lnC0-lnCt=ln(C0 / Ct) when Ct=1/2C0,t=t1/2, then t1/2=ln2/K=0.693/K First order kinetics A. eliminated at same rate per unit time B. t1/2 is a constant C. logC-T curve is linear D. steady state (Css) after 4-5 t1/2 Kinetic properties of C-T curves after single bolus injection of drug 2.3 Non-linear kinetics Higher concentration (or larger dose): zero order kinetics Lower concentration (or smaller dose): first order kinetics Because of limits in elimination capacity Examples: aspirin, phenytoin, ethanol Confirmation: different t1/2 when given different doses Michaelis-Menten kinetics dC / dt = Vmax C / (Km + C) if Km >> C dC / dt = Vmax C / Km Vmax / Km = Ke if C >> Km dC / dt = Vmax C / C dC / dt = -Vmax - First order - Zero order Kinetic properties of C-T curves after single bolus injection of drug Kinetic properties of C-T curves after single dose of aspirin 3. Pharmacokinetic models One-compartment model logC iv t 3.2 Two-compartment model 2 1 First, enter the central compartment 2, 3 Then, distributed to peripheral compartment, and eliminated Distribution Elimination t1/2 logC t1/2 iv t logC-T curve 4. Pharmacokinetic parameters and their implications 4.1 Bioavailability ( F ) Bioavailability is the fraction of administered drug (oral) that reaches the systemic circulation Absolute bioavailability(绝对生物利用度) F = AUC(po, sc, im) / AUC (iv) Relative bioavailability (相对生物利用度) F = AUC(tested) / AUC(standard) Implication: Evaluation for absorption and drug quality control Influence: Absorption rate; First-pass elimination AUC (iv) C AUC (po) t Absolute bioavailability: F = AUC(po) / AUC (iv) 4.2 Apparent volume of distribution (Vd) The volume of distribution (Vd) relates the amount of drug in the body (D) to the concentration of drug (C) in the blood or plasma. i.v. Vd = D / C p.o. Vd = FD / C 4.3 Half-life (t1/2) / elimination constant (Ke) The half-life (t1/2) is the time takes for the plasma concentration or the amount of drug in the body reduced by 50%. t1/2 = 0.693 / Ke= Vd / Cl (First-order kinetics, for most cases) Ke: A constant fraction of drug in the body is eliminated per unit of time (first-order kinetics). Implications of t1/2 Elimination rate Estimating the times of fully elimination and reaching steady state Classifying short- and long-acting drugs Adjusting dosage regimens for patients with hepatic or renal failures 4.4 Clearance (CL) The drug in a constant volume of body fluid [usually plasma] is eliminated per unit of time. (First-order kinetics) CLs = Ke Vd = FD/AUC There are also hepatic [CLH] and renal clearances [CLR]. First order kinetics lnCt = lnC0- Ke t One compartment model slope = - Ke Intravenous administration lnC0 t1/2 = 0.693 / Ke Vd = D / C0 lnCt CL = Vd × Ke slope = - Ke t (min) Part 3 Factors Influencing Drug Effects 影响药物作用的因素 Patient Drug Dosage regimen drugs, doses, intervals, duration Adjustment efficacy/adverse effects drug concentrations Doctor A. Drug Factors 1. Physic-chemical properties of drugs 2. Dose forms 3. Administration 4. Multiple-drug therapy 5. Long-term drug therapy 1. Physic-chemical properties of drugs Stability Molecular size Lipid- and water-soluble …… 2. Dose forms slow release formulation controlled release formulation transdermal patch inhalation 3. Administration Doses Routes oral intramuscular injection subcutaneous injection intravenous injection or infusion Administration time Dosing intervals Dosing duration 4. Multiple-drug therapy (drug combination) Drug-drug interactions pharmacy pharmacokinetics pharmacodynamics Drug effects in combination synergism: potentiation / addition antagonism Efficacy: ↓,↑ Toxicity: ↓,↑ B. Patient Factors 1. Physiological Factors 1.1 Age Children Sensitivity to drugs Pharmacokinetic properties Elderly Sensitivity to drugs Pharmacokinetic properties Age-related factors influencing pharmacokinetic processes 1.2 Sex Women Pregnancy - malformation and dysfunction of the fetuses Lactation - milk: effects on infants 2. Psychological Factors Placebo effects Placebo effects commonly are manifested as alteration of mood, other subjective effects, and objective effects that are under autonomic or voluntary control. 安慰剂(placebo)是指没有药理活性的物质(如乳 糖、淀粉等),被制成与试验药外观、气味相同的 制剂,作为临床对照试验中的阴性对照物。 Pharmacological effects Overall responses Non-specific drug effects Non-specific medication effects Natural recovery Absolute placebo effects No treatment Components underlying drug effects Placebo effects 3. Pathological Factors Heart diseases Hepatic diseases Renal diseases Gastrointestinal diseases Malnutrition Imbalances of acid-base or electrolytes 4. Genetic Factors Pharmacogenetics abnormality of drug responses example: tolerance of warfarin abnormality of pharmacokinetic properties example: fast or slow acetylation 5. Individual variation (个体差异) (1) Sensitivity to drugs Hypersensitivity Hyposensitivity (tolerance) (2) Abnormal responses to drugs Idiosyncracy (genetic abnormality) Allergy (immunological abnormality) One goal in the post-genomic medicine: Individualized Medicine 6. Changed responses after long-term drug use (长期用药后机体对药物反应的变化) (1) Tolerance and tachyphylaxis (human body) (2) Resistance to chemotherapy (pathogens) (3) Drug dependence - an adaptive state that develops in response to repeated drug administration. 药理学基本概念 药剂学过程 药动学过程 药学特点;用药程序 跨膜转运; 影响因素 ADME及其影响因素; 药物:理化特点, 血药浓度及动力学参数 剂型,给药方式, 联合应用 基本作用特点; 药效学过程 治疗作用与不良反应; 量效关系; 与靶分子相互作用:如受体 机体:生理、精 神、病理、遗传 因素,长期用药 后的改变 药理学基本概念 药动学过程 跨膜转运:主动转运;被动转运(含简单扩散) ADME及其影响因素: A:GI吸收/首过消除; D:血浆蛋白结合,药物理化特点,BBB M:肝药酶; E:肾排泄;胆汁排泄/肝肠循环 血药浓度及动力学参数: C-T曲线:Cmax,Tmax,AUC,Css; 房室模型:一室,二室; 速率过程:一级,零级/非线性; 药动学参数:生物利用度F, 表观分布容积Vd,半衰期t1/2,消除速率常数Ke,清除率Cl 药理学基本概念 药效学过程 基本作用特点:作用与效应;选择性 治疗作用与不良反应: 治疗作用:对因,对症,补充 不良反应:副反应,毒性反应,变态反应,后遗效应,特异质反应等 量效关系:效能,效价强度,治疗指数 ( TI = LD50 / ED50 ) 与靶分子相互作用(特异性作用机制): 受体:亲和力,内在活性,激动药,拮抗药,部分激动药 药理学基本概念 影响因素 药物因素:理化特点,剂型,给药方式; 联合应用:协同、拮抗,有利、有害 机体因素: 生理:年龄、性别等 精神:安慰剂效应等 病理:肝、肾、胃肠道功能,疾病状态等 遗传:药物代谢、效应的个体差异 长期用药后的改变:耐受/快速耐受,耐药,依赖性/成瘾 思考题 一个催眠药口服后,从给药后到作用发挥和作用消除, 在体内经历哪些过程? 你认为药物作用基本规律主要有哪些方面? 为什么血浆白蛋白及体内各种酶不能称为药物受体? 怎么理解药动学基本过程(ADME)和药动学参数的关 系? 药物血浆消除半衰期(t1/2)在临床应用中有何意义?